

- Date:
- 5 Dec 2023
Our workforce, our future sets out the collective knowledge, skills and ways of working the mental health and wellbeing workforce needs to deliver quality care, support and treatment.
The framework puts consumers, carers, families, and supporters at the centre of care. It also acknowledges and values the breadth of expertise and experience across the workforce.
First released in December 2021, Our workforce, our future (previously known as the Mental Health and Wellbeing Workforce Capability Framework) provided an overview of the principles and capabilities required of the multidisciplinary and evolving workforce. It was developed in response to recommendation 58 of the Royal Commission into Victoria’s Mental Health System.
This revised version includes further detail to support different roles and levels within the mental health and wellbeing workforce. It also includes outcome statements and information to support reflective practice.
Our workforce, our future will be used to inform workforce development planning, enhance professional learning delivery and support the design of multidisciplinary teams across the mental health and wellbeing sector.
Foreword: Our workforce, our future
Victoria's mental health workforce is at the heart of our mental health and wellbeing system – a fact recognised by the Royal Commission into Victoria’s Mental Health System.
The Royal Commission’s final report recommended a number of workforce reforms to ensure that our workforce has the right:
- size, diversity and distribution across the state
- support for their practice
- capabilities for the future.
These recommendations include developing this mental health and wellbeing workforce capability framework, which will apply to the whole of the workforce across roles, professions and settings.
The framework supplements current and future workforce initiatives underpinning system reforms that will build the new, responsive and integrated Victorian mental health and wellbeing system envisioned by the Royal Commission.
The practice principles in the framework are intended to support implementation of the principles of the new Mental Health and Wellbeing Act 2022, reflecting the recommendations of the Royal Commission. They focus on human rights, respectful, compassionate and collaborative practice, and understanding the diverse needs of individuals and their families and carers.
The framework sets out the collective knowledge, skills and ways of working our workforce needs to deliver quality care, support and treatment.
The framework puts consumers, carers and families at the centre. It also acknowledges the breadth of diverse expertise and experience across the mental health and wellbeing workforce. It recognises and values all forms of expertise equally.
This first version of the framework is the beginning of a conversation. It is a platform from which further reflection and innovation will occur at individual, team, service and system levels to inform future iterations.
We invite every Victorian mental health and wellbeing professional, team, service leader, educator, training organisation and other system stakeholders to embrace, use and build upon the framework. Together, we can build a mental health and wellbeing service system with a culture of collaboration, curiosity, continuous learning and care.
Translating the framework into practice and creating meaningful change rests in our collective hands. The more the workforce is supported to develop its capabilities in line with this new framework, the better equipped it will be to enact the principles and requirements of the new Mental Health and Wellbeing Act 2022.
As we continue this reform journey together, the framework represents a foundational tool to support a more reflective and collaborative approach in the way we think about capability development in the new, responsive and better integrated mental health and wellbeing system.
Professor Euan Wallace AM
Secretary, Department of Health
Introduction to the capability framework
The framework is a foundational resource for Victoria’s mental health and wellbeing workforce.
This first iteration of the framework sets out the knowledge, skills and ways of working that our diverse, multidisciplinary and evolving workforce needs.
It provides a common language for all members of the mental health and wellbeing workforce in both direct care roles and support functions – regardless of professional discipline, background, role and setting.
Ultimately, it seeks to generate a sense of collective identity and reciprocal responsibility for how we deliver care, support and treatment in Victoria’s mental health and wellbeing system.
Background and development
The framework is developed on the recommendations of the Royal Commission into Victoria’s Mental Health System and the input received during its 2019–2021 inquiry.
Purpose and objectives
The framework sets out the knowledge, skills and ways of working required to effectively deliver care, support and treatment in the mental health and wellbeing system.
How the framework supports mental health reform
A diverse, skilled and multidisciplinary workforce is at the heart of the Royal Commission’s vision for a reformed mental health and wellbeing system.
Alignment with other frameworks and standards
The framework sits alongside professional discipline and service-specific requirements and capability frameworks.
How to use this framework
The framework is for individual members of the workforce, service leaders, organisations, and institutions that engage with the system.
Background and development
The framework has been developed following the recommendations of the Royal Commission into Victoria’s Mental Health System and the many contributions received through the course of its inquiry undertaken between 2019–2021.
This includes thousands of submissions and witness statements, a wide range of sector and community consultations and a frontline mental health and wellbeing workforce survey.
The Victorian Department of Health then undertook a series of targeted consultations with frontline professionals from diverse backgrounds, roles and settings, as well as lived experience representatives, subject-matter experts, service leaders and professional bodies to test and refine the framework.
The Department’s Workforce Technical Advisory Group and Lived Experience Advisory Group supported this engagement. The framework is the result of all these efforts, and the many valuable contributions from individuals and organisations.
Purpose and objectives
The framework sets out the knowledge, skills and ways of working required to effectively deliver care, support and treatment in the mental health and wellbeing system, now and into the future. It provides a common language that can be used across professions, disciplines, specialties and roles to encourage an inclusive, shared approach to professional practice.
It aims to:
- support members of the workforce – regardless of professional discipline, background or setting – to understand what the knowledge, skills and attributes (capabilities) they need to meet the responsibilities of their role
- empower teams to consider their collective skills and expertise and how best to use them to support positive health and wellbeing outcomes for consumers, families, carers and supporters
- support educators, managers and leaders to plan, develop and invest in professional development and learning
- support educators, managers and leaders with workforce planning, recruitment and career development
- inform strategic workforce planning, including recruitment, induction, and retention
- inform and guide responses to research and gaps in workforce capabilities
- support monitoring and evaluation of activities designed to develop and embed workforce capabilities
- support the design of balanced, multidisciplinary teams that meet the needs of consumers, service settings and context.
Ultimately, the framework will support our workforce to use its individual and collective skills and expertise to deliver better multidisciplinary practice across the Victorian mental health and wellbeing system.
How the framework supports mental health reform
A diverse, skilled and multidisciplinary workforce is at the heart of the Royal Commission’s vision for a reformed mental health and wellbeing system – a system that supports better outcomes for consumers, families, carers and supporters.
The workforce will play a vital role in driving continuous improvement of the system as we seek to work in new ways across different settings.
The reformed mental health and wellbeing system will bring together our workforce’s expertise to deliver evidence-informed care, support and treatment in collaborative ways, within and across services. All forms of expertise will be valued and respected, including lived experience expertise, as well as other unique contributions from different disciplines.
To realise the full potential of genuine multidisciplinary, integrated and collaborative practice, we need to work in new ways. We need to transform our workforce’s cultures, and create more nuanced, holistic and person-centred approaches and capabilities across the system.
These system-wide reforms, including commencement of the Mental Health and Wellbeing Act 2022 will involve new and integrated models of care and service design that respond to the needs of consumers, families, carers and supporters. This will entail creating new roles and changing workforce composition.
The framework values and recognises all forms of expertise, experience, knowledge and skills that already exist within the mental health and wellbeing system. It will support the workforce to evolve and expand upon existing capabilities to realise the vision of an integrated and collaborative system. It will support a common understanding of the knowledge and skills needed to achieve positive outcomes for all consumers, families, carers and supporters.
This first iteration of the framework is the beginning of a conversation. It represents a point in time in the early stages of a 10-year reform journey towards the future integrated and responsive mental health and wellbeing system. We will revise and review it to keep pace with the emerging and evolving needs of a complex and diverse system.
Ultimately, the framework aims to support the transformation of the mental health and wellbeing system. It seeks to harness the passion of the workforce to create better outcomes for all by building collaborative, compassionate relationships with consumers, families, carers and supporters.
Alignment with other frameworks and standards
The framework sits alongside professional discipline and service-specific requirements and capability frameworks.
It seeks to support multidisciplinary and collaborative practice across roles and settings, by supporting knowledge and skills to be developed in more consistent ways from a single point of reference.
The principles of the capability framework align with those in the Mental Health and Wellbeing Act 2022 and provide the workforce with practical guidance on how to enact the principles in their work.
It does not replace existing profession or discipline-specific standards, guidelines or training protocols. Table 1 shows the documentation for some of the relevant mental health and wellbeing workforces.
Alignment with other frameworks and professional standards
| Workforce | Frameworks and standards |
|---|---|
| Aboriginal health and/or mental health practitioners |
|
| AOD workers |
|
| Carer or family peer workers |
|
| Case managers |
|
| Consumer peer workers |
|
| Counsellors |
|
| Emergency services |
|
| Lived experience workers |
|
| Medical practitioners |
|
| Occupational therapists |
|
| Nurses |
|
| Psychiatrists |
|
| Psychologists |
|
| Social workers |
|
While the framework focuses on shared capabilities across the entire workforce, we know that certain service settings and consumer cohorts will need tailored approaches.
We also understand that the people who use the mental health and wellbeing system also engage with other parts of the broader healthcare and social services system – including but not limited to disability, children and families, justice, family violence and education. Members of these other workforces, particularly those working as part of multidisciplinary teams, will draw on the capabilities set out in this framework.
How to use this framework
The framework is for individual members of the workforce, service leaders, organisations, and institutions that engage with the system.
It aims to support reflection, growth and development at all these levels.
The ultimate goal is to improve the experience for consumers, carers and families. We want to ensure that all Victorians have positive mental health and wellbeing outcomes.
For members of the workforce, the framework helps you undertake reflective practice. You can use it to self-assess your knowledge and skills. You can also use it to discuss capability development with your peers, team leaders, supervisors and managers.
For service leaders, the framework helps you determine professional development priorities, as well as create diverse teams, and assess team capabilities so you can take advantage of group learning opportunities. It also provides approaches to professional practice supervision, and supports growth and career pathways.
For organisations, the framework supports values-based recruitment, team composition and role descriptions, and career development. It sets out how individuals and organisations need to adapt, grow and continuously improve to achieve the highest standards of practice.
For institutions, such as education and professional bodies, the framework will guide the development of education, training programs and curriculum. It complements or informs professional development requirements for formal or informal accreditation. You can use it to review standards of practice to provide another layer of insight and consistency.
The capability framework provides reflective practice questions that can help you develop your practice.
Here are some examples of the ways different members of the workforce can use the capability framework:
- As a frontline worker, I will use the capability framework, along with my experience, education and other learning, to inform the way I work with consumers, families, carers and supporters. The framework will help me to work collaboratively with colleagues within and across services.
- As a consumer peer-support worker, I will use the capability framework to guide my interactions with consumers and with colleagues in multidisciplinary teams. This will help me provide safe and effective peer support.
- As a training or education provider for the sector, we will use the capability framework to guide design, delivery and continuous improvement of our curriculum. We understand the need for consistent practice across the sector, and we will align our learning and development training and resources with the principles and capabilities set out in the framework.
- As a family peer-support worker, I will use the capability framework to guide my interactions with families, carers and supporters, as well as to guide how I work with colleagues in multidisciplinary teams. The framework will help us all recognise that families and carers have their own support needs too.
- As a practice supervisor and mentor for the team, I will use the capability framework to guide my reflective practice. I will use it to prepare development plans and assess progress against performance goals. The framework will also help me understand the skills and knowledge the team needs to deliver effective care, support and treatment.
- As a people manager, I will use the capability framework to support workforce planning, and to understand the capabilities that I need to recruit for and continually develop and assess. This will ensure that our organisation has the right mix of capabilities to deliver positive mental health and wellbeing outcomes for all people and their families, carers and supporters.
- As a service leader, I will use the capability framework to support the recruitment and professional development of my team. The framework will help me understand and communicate the approaches and capabilities our organisation needs to deliver effective outcomes.
- As someone with lived experience of mental illness, I will use the capability framework to understand the expectations of this role in the sector, as well as the capabilities I will need to develop throughout my career.
Structure of the capability framework
The framework includes three core components: safe and supportive working environments, principles, and capabilities.
The capability framework supports our workforce to understand and respond to the needs of consumers, families, carers and supporters at every point of care. It does this by setting out shared principles and capabilities.
The framework includes three core components: safe and supportive working environments, principles, and capabilities. Each of these puts the needs of consumers, families, carers and supporters at the centre of the mental health and wellbeing system.
Safe and supportive working environments
A safe and supportive working environment is the foundation and prerequisite for all members of the workforce to use their existing capabilities effectively.
Principles
Our workforce shares common values, approaches, attitudes and ways of working with consumers, families, carers, supporters and colleagues – both within and across services. The framework sets out seven principles to guide our practice, regardless of setting, role or level of specialisation.
Capabilities
The framework also sets out 15 capabilities that outline the knowledge and skills required to deliver safe and effective care, support and treatment.
Capabilities are described for:
- whole-of-workforce – all workers who interact with consumers, families, carers and supporters within and intersecting with the mental health and wellbeing system. This includes support and administration staff, and workers who support mental health and wellbeing learning, development and broader sector engagement
- care, support and treatment professionals – those involved in the direct provision of mental health and wellbeing care, support and treatment for consumers, families, carers and supporters
- technical or specialist professionals – those who have specialist and technical skills within the described capability, which may include technical and specialist expertise in one or more areas of that capability domain but not necessarily all areas
- leadership – team managers and service leaders across a variety of service functions and settings, inclusive of those in auxiliary services such as education institutions, peak bodies and unions.
A safe and supportive working environment
This capability framework seeks to build cultures of curiosity, collaboration and care through evidence-informed practice.
A safe and supportive working environment is at the centre of effective practice, capability development, and sustainable, lifelong careers for our workforce.
Cultures of curiosity, collaboration and care
It takes great dedication, compassion and strength to work in the mental health and wellbeing sector.
As a workforce, you told us how important it is for you to feel empowered, trusted and respected in your daily work. You told us you want to feel safe and supported in your roles, with enough time for reflective practice and professional practice supervision. You told us you want to have the right balance of time with consumers alongside other responsibilities.
In addition, the Royal Commission emphasised that an effective workforce needs a mental health and wellbeing system that:
- encourages and supports excellence, and values all types of expertise – including lived experience expertise
- enables the workforce to use existing capabilities, and develop skills and knowledge to continually improve the quality of treatment, care and support
- ensures the workforce feels safe, trusted, respected and valued
- ensures the Victorian mental health and wellbeing system is an attractive, contemporary and sustainable place to work that supports workforce wellbeing and career progression.
We also know that to create safe and supportive working environments, our workforce needs good physical working environments, with robust occupational health and safety, effective supervision and allocation of resources.
Some workforce groups face additional challenges. These include those working in rural and isolated services, lived experience workforces and workforces with diverse identities such as Aboriginal practitioners, LGBTIQ+ practitioners and culturally diverse practitioners. We know we will need tailored approaches to create safe and supportive working environments for these workforce cohorts.
This capability framework helps service providers, organisations, workforce professional bodies, educators and others to support the wellbeing and safety of the mental health workforce. It seeks to build cultures of curiosity, collaboration and care through evidence-informed practice.
If we wish to provide a recovery-oriented, compassionate experience for consumers, carers, families and supporters, we need to do the same thing for our workforce. We need to create working environments that make our workforce feel safe, respected and valued for the expertise you bring to your work. This will allow our workforce to build knowledge, skills and collaborative ways of working with each other as well as consumers, families, carers and supporters.
Principles
The common values, approaches, attitudes and ways of working that guide all practice.
The seven principles provide a common set of core values and approaches that underpin all interactions between professionals and consumers, carers and families.
Seven practice principles
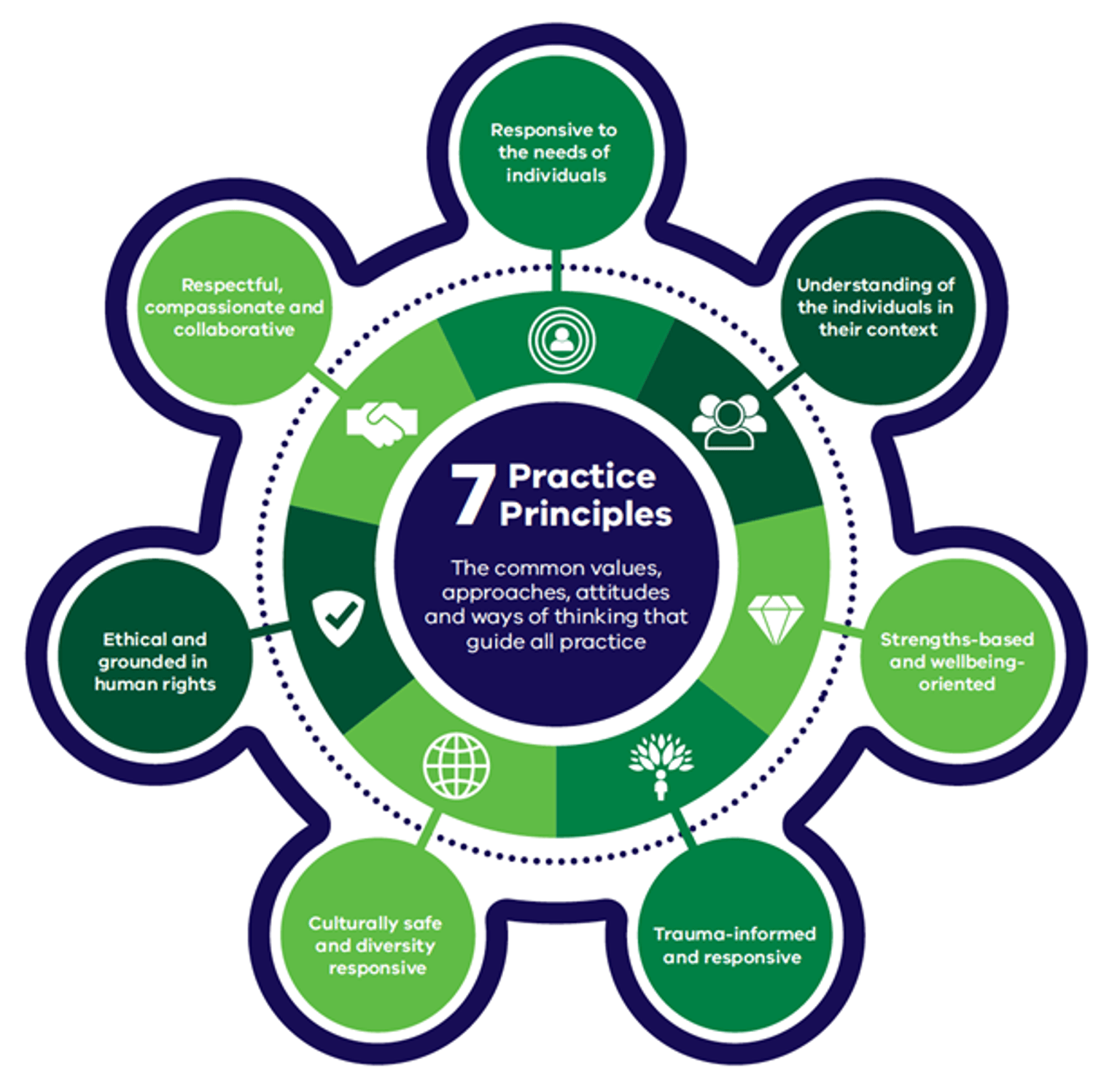
{kind=link}
Capabilities
The knowledge and skills required to deliver safe and effective care, support and treatment in the Victorian mental health and wellbeing system.
The Our workforce, our future capability framework outlines the knowledge and skills required to deliver safe and effective care, support and treatment in the Victorian mental health and wellbeing system.
This framework organises the capabilities into domains that represent key areas of practice in the mental health sector.
We consider these capabilities from the perspectives of the consumer, family, carer and workforce, to ensure that practice remains person-centred. Each capability also includes a collective outcome.
Taken together, the capabilities aim to strengthen and support the Victorian mental health workforce to be able to meet the needs of consumers, families, carers and supporters into the future.
15 capabilities
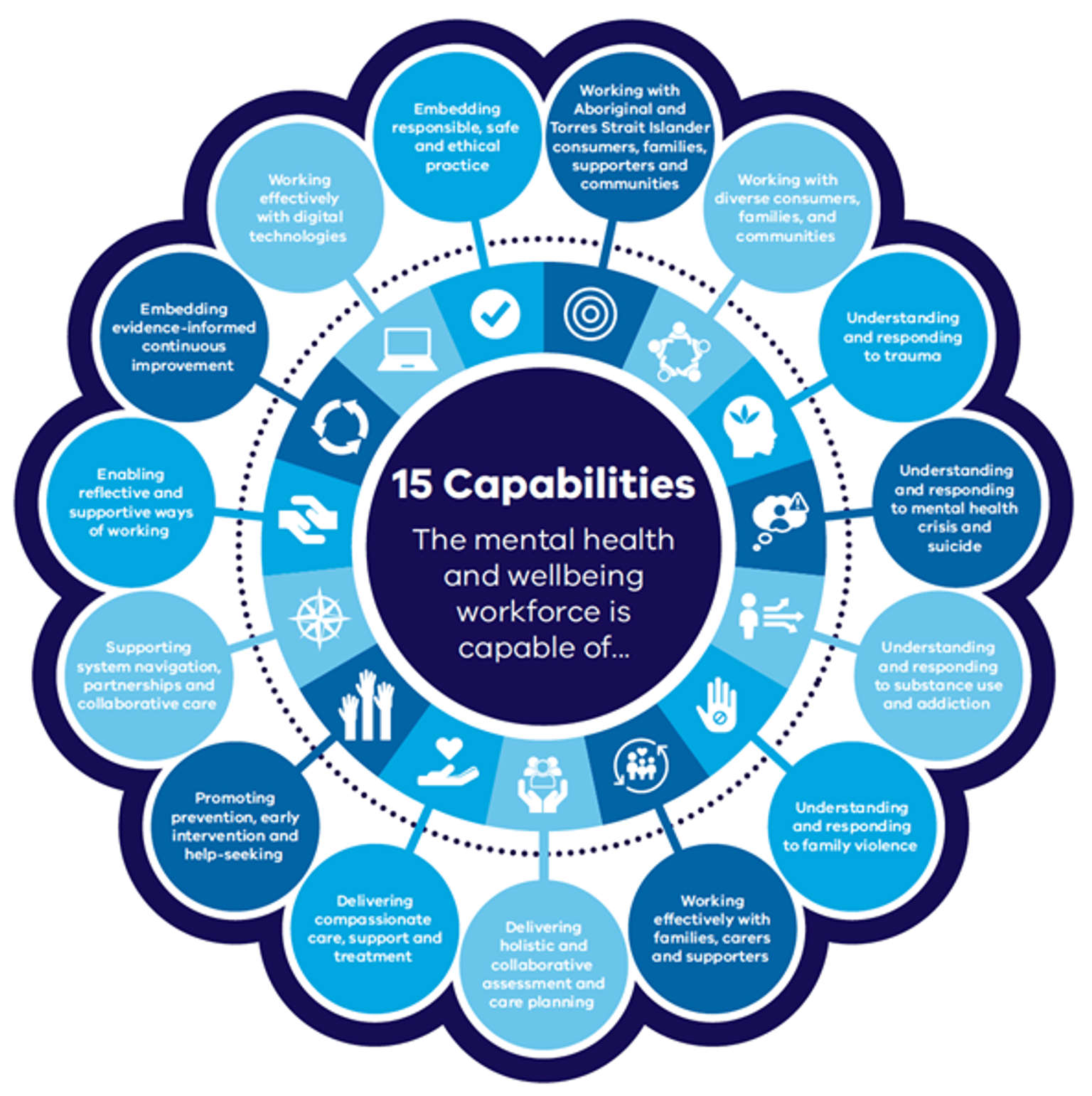
{kind=link}
Our workforce, our future pathways tool
You can assess your knowledge of the capabilities using the Our workforce, our future pathways tool.
This specially developed tool has been designed to help the mental health workforce explore and deepen their understanding of the 15 capabilities outlined above.
Use it to take your skills to the next level and help you assess your capabilities for delivering mental health and wellbeing services, identify areas for growth, and uplift your expertise to deliver better outcomes for consumers, carers, families and supporters.
Access the pathways tool on the MHPOD Learning Portal.
Glossary: Our workforce, our future
Definition of key terms used in the capability framework for the mental health and wellbeing workforce.
This glossary defines key terms used in this framework. These definitions are indicative and may not reflect the ‘dictionary definition’ of each term. These terms are deliberately aligned with definitions used by the Royal Commission in order to further promote the vision and values of the reforms.
Term |
Intended definition |
|
care, support and treatment |
We use this term to show that care, support and treatment are fully integrated, equal parts of the responses in the mental health and wellbeing system. This includes wellbeing supports, such as rehabilitation, wellbeing and community participation, that are a key part of supports and responses. |
|
carer |
This is a person, including a person under the age of 18 years, who provides care to another person with whom they are in a relationship of care. |
|
compassion |
Compassion refers to the feeling that arises when a person is confronted with another's suffering and feels motivated to relieve that suffering. Compassion literally means ‘to suffer together’. It is different from empathy or altruism, although the concepts are related. |
|
consumer |
This is a person who identifies as having a lived living or living experience of mental illness or psychological distress, irrespective of whether they have a formal diagnosis, who has used mental health services and/or received treatment. |
|
empathy |
Empathy is the ability to sense other people's emotions, coupled with the ability to imagine what someone else might be thinking or feeling. |
|
expert |
An expert is a person who is known for their specialist knowledge and/or skills in a particular area. |
|
family |
This may refer to family of origin and/or family of choice. |
|
family violence |
Family violence is any violent, threatening, coercive or controlling behaviour that occurs in current or past family, domestic or intimate relationships. |
|
holistic |
This means viewing the person as a whole, taking into account things such as social determinants of health and wellbeing, and how these influence and interact with each other. |
|
lived experience |
People with lived experience identify either as someone who is living with (or has lived with) mental illness or psychological distress, or someone who is caring for or otherwise supporting (or has cared for or otherwise supported) a person who is living with (or has lived with) mental illness or psychological distress. People with lived experience are sometimes referred to as ‘consumers’ or ‘carers’, acknowledging that the experiences of consumers and carers are different. |
|
lived experience workforce |
The lived experience workforce is a broad term used to represent two distinct professional groups in roles focused on their lived expertise: • people with personal lived experience of mental illness (‘consumers’) • families and carers with lived experience of supporting a family member or friend who has experienced or is experiencing mental illness. There are various paid roles among each discipline. This includes workers who provide support directly to consumers, families and carers through peer support or advocacy, or indirectly through leadership, consultation, system advocacy, education, training or research. |
|
leadership role |
A leadership role is one which sets direction for others, who manages or leads others, or who has influence and accountability over decision-making in relation to mental health and wellbeing supports, systems, practices and delivery. |
|
mental health and wellbeing |
This describes an optimal state of mental health, including as it relates to people with lived experience of mental illness or psychological distress. It can also be used to refer to the prevention, avoidance or absence of mental illness or psychological distress. |
|
mental health and wellbeing system |
The Royal Commission outlined a vision for the future mental health and wellbeing system, which will be designed over the short to medium term. As such, the definition of the mental health and wellbeing system will evolve alongside the reforms. However, it should include the strengths and needs that contribute to people’s wellbeing, alongside hospital-based and community care, support and treatment. |
|
multidisciplinary teams |
Multidisciplinary teams bring together the expertise and skills of different workforces, roles and professionals (including those with lived and living experience). For the purposes of this framework, a multidisciplinary team is one that involves diverse expertise, and in which all expertise is valued, in order to provide care, support and treatment collaboratively and compassionately. |
|
peer |
A peer is someone who shares the same status, skills or other attribute or position. |
|
peer-support workers |
Peer-support workers use their own recovery experiences to support others to navigate their recovery journeys. |
|
professional cohorts |
Professional cohorts refer to group/s that align based on professional accreditation, experiences and/or expertise. |
|
recovery |
Recovery is defined by the person and refers to an ongoing holistic process of personal growth, healing and self-determination. As an ongoing journey of personal growth and wellbeing, the notion of recovery does not equate with a particular model of care, phase of care or service setting. |
|
reflective practice |
Reflective practice is a process of learning through and from experience to gain new insights via: • reflection on experiences of delivering care, treatment and support to consumers, families, carers and supporters • examining and critically reflecting on assumptions underlying everyday practices • reflecting on challenging interpersonal dynamics. |
|
secondary consultation |
Secondary consultation is a discussion between mental health clinicians about a particular consumer. This can enable different care providers to work collaboratively to discuss issues with the consumer’s care. Other models of secondary consultation focus on the needs of consumers more generally – for example, consumers with particular mental health needs or a specific diagnosis. This model focuses on sharing knowledge and expertise between different care providers. |
|
self-determination |
In a collective sense, this term is used to refer to the ‘ability of Aboriginal peoples to freely determine their own political, economic, social and cultural development as an essential approach to overcoming Indigenous disadvantage’. This can be applied more broadly to any person’s ability to determine their own development. |
|
social determinants of mental health |
A person’s mental health and many common mental illnesses are shaped by social, economic, and physical environments, often termed the ‘social determinants of mental health’. Risk factors for many common mental illnesses are heavily associated with social inequalities, whereby the greater the inequality, the higher the inequality in risk. |
|
social and emotional wellbeing |
Social and emotional wellbeing refers to being resilient, being and feeling culturally safe and connected, having and realising aspirations, and being satisfied with life. This is consistent with Balit Murrup, Victoria’s Aboriginal social and emotional wellbeing framework. |
|
substance use, gambling and addictive behaviours |
Substance use means the use of alcohol, tobacco or other drugs (prescription or illicit). Substance use may become harmful to a person’s health and wellbeing or can have other impacts on someone’s life or that of their family and broader social network. Addictive behaviours, including gambling, means compulsive behaviours outside of a person's control, even when it has harmful effects on that person or their family. |
|
supported decision-making |
This is the process that supports a person to make and communicate decisions with respect to personal or legal matters. This may be achieved by offering consumers access to a variety of tools and resources such as non-legal advocates and peer worker. |
|
trauma-informed |
Trauma-informed approaches recognise the possibility of the ongoing effects of past and current trauma in the lives of everyone seeking support and how this can affect the way people seek help. |
|
victim survivor |
Describes people – including adults, children and young people who have direct firsthand experience of family violence, as well as immediate family members of those who have lost their lives to family violence. This term acknowledges the ongoing effects and harm caused by abuse and violence as well as honouring the strength and resilience of people with lived experience of family violence. |
Guides and resources
Access a range of resources to help your workforce embed Our workforce, our future: a capability framework for the mental health and wellbeing sector.
Our workforce, our future sets out the collective knowledge, skills and ways of working for the mental health and wellbeing workforce in Victoria.
Implementing the capability framework into practice will help strengthen the workforce.
It will ensure they are well-equipped to continue providing high-quality care to consumers, families, carers and supporters.
A range of resources have been developed to help organisations and workers implement the framework.
Implementation guide
This is a guide to support the sector in embedding the principles and capabilities of Our workforce, our future. This guide can help you align your workforce development practices with the framework’s vision. It provides practical steps and strategies, as well as tools and resources to adopt the framework.
Pathways tool
The Our workforce, our future pathways tool has been developed to help the mental health workforce explore and deepen their understanding of the 15 capabilities outlined in the Our workforce, our future capability framework. It's been designed to assist workers in the mental health sector to assess their capabilities in delivering mental health and wellbeing services, identify areas for growth, and uplift your workforce to deliver better outcomes for consumers, carers, families and supporters.
The learning journey for each capability incorporates three components:
- A series of micro learning videos where people can learn more and hear from practitioners, mental health professionals, Lived and Living Experience workers and consumers and carers.
- A skills-gap analysis to rate their level of confidence in a capability or skill, and the level they would like to reach.
- Access to curated resources to further develop their knowledge and skills of each capability.
The tool can be accessed on the MHPOD Learning Portal.
Ask AI about Our workforce, our future
The Ask AI tool makes it easier to access and understand the capabilities and skills needed to provide best-practice mental healthcare.
It’s capable of answering a number of questions, ranging from “How do I adapt my practice to be culturally safe?” to “How do I recognise and respond to trauma effectively?”
All responses are drawn from the Our workforce, our future capability framework, and include references to resources for users to delve into.
Explore example questions and answers by selecting the ‘Getting Started’ tab at Ask AI, to see how the new tool can support your practice.
Organisational Assessment Tool
The Organisational Assessment Tool can help mental health and AOD organisations to evaluate how well they are set up to support workforce development.
The tool can be used to identify strengths, gaps and opportunities across key areas of practice and includes a suite of practical resources.
It also includes a step-by-step guide to help teams choose the most relevant resources, based on their role and the priorities of their health service.
The Organisation Assessment Tool ensures organisations can build their workforce’s capability in a targeted, sustainable and meaningful way.
Supporting people experiencing a mental health issue who are justice involved
This companion guide supports the mental health and wellbeing workforce to provide safe, effective and compassionate care to people who are justice-involved or at risk of offending.
Developed by Forensicare, it can be used by people across a range of roles - from frontline practitioners to service leaders. It outlines the knowledge, skills and behaviours needed to respond to the complex needs of this population.
The guide is a practical tool to help build workforce capability, reduce stigma, and improve outcomes for some of Victoria’s most marginalised and vulnerable consumers.
The Infant, Child, Youth and Family Companion Guide
This guide offers tailored support for people working with infants, children, young people and families across Victoria’s mental health and wellbeing system.
Developed by Mindful at the University of Melbourne, it identifies the specific skills, knowledge and approaches needed to work effectively with people up to 26 years old.
It’s a practical resource for clinicians, educators, leaders and support staff to help them deliver appropriate, inclusive and compassionate care.