

The Our workforce, our future capability framework outlines the knowledge and skills required to deliver safe and effective care, support and treatment in the Victorian mental health and wellbeing system.
This framework organises the capabilities into domains that represent key areas of practice in the mental health sector.
We consider these capabilities from the perspectives of the consumer, family, carer and workforce, to ensure that practice remains person-centred. Each capability also includes a collective outcome.
Taken together, the capabilities aim to strengthen and support the Victorian mental health workforce to be able to meet the needs of consumers, families, carers and supporters into the future.
15 capabilities
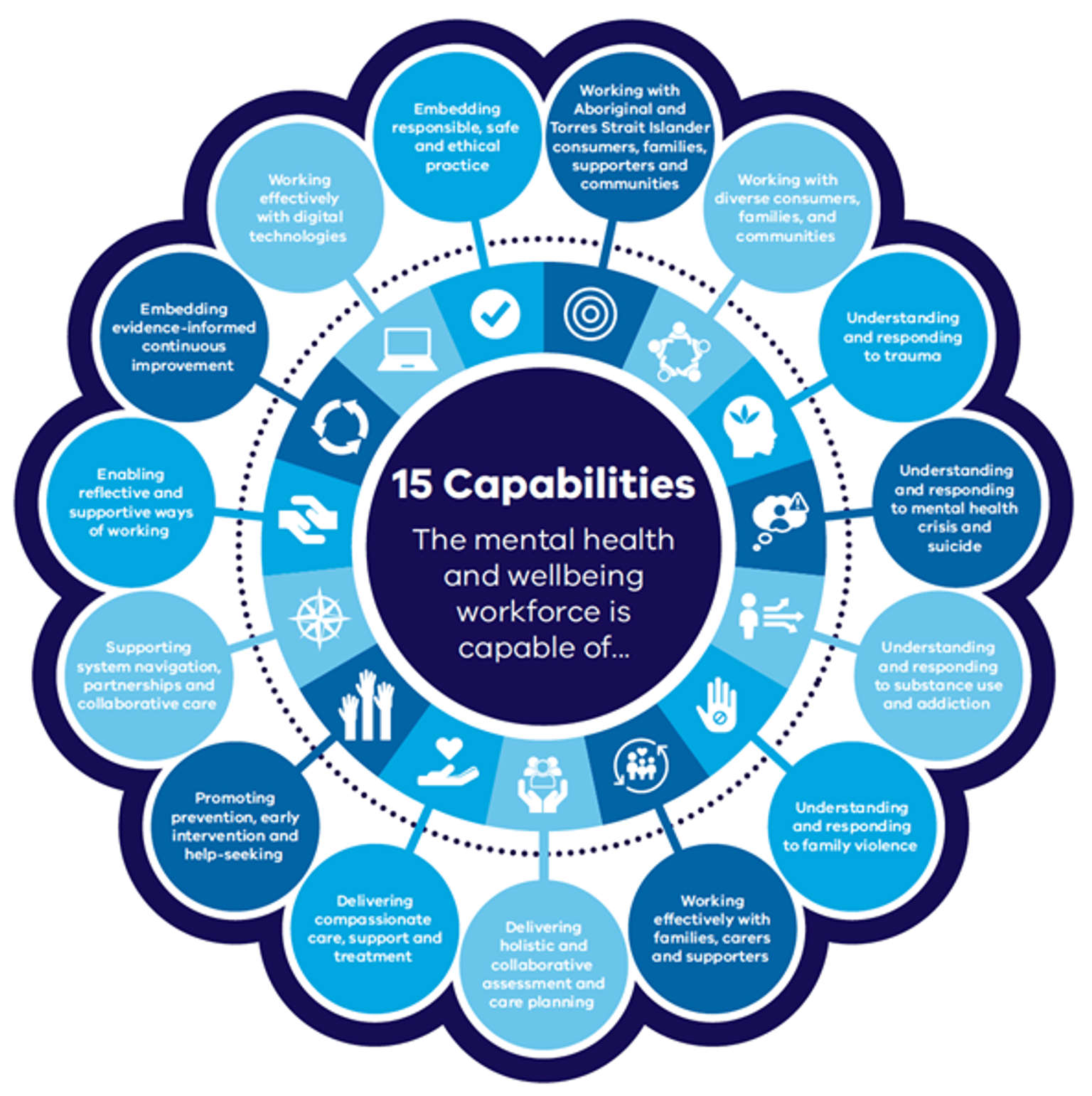
15 Capabilities
- Embedding responsible, safe and ethical practice
- Working with Aboriginal consumers, families, and communities
- Working with diverse consumers, families, and communities
- Understanding and responding to trauma
- Understanding and responding to mental health crisis and suicide
- Understanding and responding to substance use and addiction
- Understanding and responding to family violence
- Working effectively with families, carers and supporters
- Delivering holistic and collaborative assessment and care planning
- Delivering compassionate care, support and treatment
- Promoting prevention, early intervention and help-seeking
- Supporting system navigation, partnerships and collaborative care
- Enabling reflective and supportive ways of working
- Embedding evidence-informed continuous improvement
- Working effectively with digital technologies
- Download '15 capabilities'
{kind=link}
Our workforce, our future pathways tool
You can assess your knowledge of the capabilities using the Our workforce, our future pathways tool.
This specially developed tool has been designed to help the mental health workforce explore and deepen their understanding of the 15 capabilities outlined above.
Use it to take your skills to the next level and help you assess your capabilities for delivering mental health and wellbeing services, identify areas for growth, and uplift your expertise to deliver better outcomes for consumers, carers, families and supporters.
Access the pathways tool on the MHPOD Learning Portal.
Care, support and treatment is consistent with professional, legal and ethical codes of conduct and practice. It respects and protects the preferences and rights of consumers, families, carers and supporters. All interactions, including supported decision-making, are consistent with human rights frameworks.
Outcome statements
Consumer outcome statement
My care, support and treatment is ethical at all times. My rights are respected, upheld, promoted and communicated clearly to me. My dignity is actively ensured. I am responded to with compassion. I am supported to seek redress when this does not occur.
Carer and family outcome statement
Our rights are respected, upheld and communicated clearly to us. Our contribution and perspective is valued. We are considered and engaged throughout care. We are responded to with dignity and compassion. Our safety is prioritised at all times. We are supported to seek redress when this does not occur.
Workforce outcome statement
We work within national, professional, legal and local codes of conduct, practice and legislation as required by our role and discipline.
We uphold and communicate the rights of consumers, families, carers and supporters in every interaction with the system. We empower people to make informed decisions that promote their safety and wellbeing.
We are a respected and valued workforce. Our workplace is safe and supportive. We are supported to seek redress when this does not occur.
Collective outcome statement
Together, we contribute to an ethical mental health and wellbeing system that respects and upholds the rights of everyone. We are all informed about and understand how to seek redress when this does not occur. Redress and complaints processes are trauma-informed and underpinned by human rights. These processes lead to a safer, fairer system.
Key knowledge and skills
Whole mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- current and emerging human rights frameworks and practices
- that human rights include, but are not limited to, the right to autonomy and self-determination, safety, freedom from coercion, and treatment in a non-discriminatory and minimally restrictive way
- current legislation, frameworks, guidelines, policies and codes of practice that relate to delivering safe and responsive care to consumers, families, carers, supporters and communities
- concepts of confidentiality, informed consent, privacy and information sharing, and the associated practice implications.
The mental health and wellbeing workforce will:
- promote, respect and protect the rights and responsibilities of consumers, families, carers and supporters
- remove barriers that limit people’s rights
- maintain a current understanding of, and commitment to, a human rights framework
- maintain a current understanding of, and commitment to, the scope of practice set out by national, professional, legal and local codes of conduct and practice
- promote supported decision-making, self-determination and choice
- advocate for and create safe and healing spaces
- challenge stigmatising attitudes, discrimination, and exclusion
- work to reduce and eliminate restrictive practices.
Care, treatment and support roles
Those in care, support and treatment roles will:
- practise ethically
- uphold the rights of consumers, families, carers and supporters
- apply concepts of self-determination, privacy and confidentiality, consent and information sharing, and understand and manage the associated practice implications
- ensure that consumers, families, carers and supporters actively shape their care, support, and treatment
- respect, protect and promote individual choice and actively facilitate supported decision-making
- adopt and advocate to reduce restrictive approaches to care
- work in ways that actively protect consumers, families, carers and supporters from violence, abuse and exploitation
- report incidences of violence, abuse and exploitation in line with guidelines and legislation
- work within their capability and demonstrate awareness of when and how to seek additional support.
Technical or specialist roles
Those in technical or specialist roles will:
- deliver or provide expert guidance and direction on ethical and supported decision-making
- deliver or provide expert guidance and direction on safe and informed risk-taking, promoting autonomy and choice
- deliver or provide expert guidance and direction on safe de-escalation techniques and responses to aggression and violence
- provide expert guidance and direction to support understanding and application of mental health and other legislation
- provide expert guidance and direction on the applicability and practice implications of relevant legal and human rights for consumers, families, carers and supporters
- provide expert guidance and direction on the human rights implications of approaches to care, support and treatment, and champion ethical, safe and responsive practice and approaches.
Leadership roles
Those in leadership roles will:
- embed ethical and human-rights informed ways of working
- embed active and ongoing reflective practice focused on responsible, safe and ethical practice
- provide meaningful opportunities for ongoing learning that promotes ethical, safe and responsive care, support and treatment
- embed safe and supported accountability mechanisms (for example, feedback and complaints processes) to ensure care, support and treatment is ethical, safe and responds to the needs and preferences of consumers, families, carers and supporters
- actively work towards the elimination of seclusion and restraint
- advocate for continuous improvement of the mental health and wellbeing system
- lead by example by delivering and demonstrating responsible, safe and ethical workspaces for all.
Reflective practice questions
- How have I supported those I am working with to understand their rights and responsibilities?
- How can I further develop my skills to ensure responsible, safe and ethical practice?
- How have I used the concept of proportionality to ensure I am giving proper consideration to human rights, and acting compatibly with them, when making decisions?
Care, support and treatment enables Aboriginal consumers, families, supporters and communities to achieve resilience, self-determination and empowerment. It also promotes a sense of identity and belonging. Collaboration with Aboriginal people requires a holistic view of Aboriginal social and emotional wellbeing, where connectedness and relationships are central. This includes connection to Country and culture, spirituality and ancestors, family and community. It also recognises the influence of past experiences, broader social factors and physical health on wellbeing.
Outcome statements
Consumer outcome statement
My understanding of wellbeing is respected, supported and central to all engagement. This includes my connection to spirituality, ancestors, land, culture, community, family, kinship, mind, emotions and body. I am empowered to make decisions about the care, support and treatment that is right for my social and emotional wellbeing.
Carer and family outcome statement
Our connection as family, kin and community informs the understanding of social and emotional wellbeing. Care, treatment and support follows the principles of self-determination. We are considered and included in the care and treatment of the person we support.
Workforce outcome statement
We consider the broad dimensions of social and emotional wellbeing, prioritising Aboriginal self-determination.
We embrace culturally responsive practices and use preferred language. We work respectfully with Aboriginal people, in line with relevant local, state and national guidelines, policies and frameworks.
We are committed to decolonising our practice. We recognise the resilience and wisdom of Aboriginal people and communities. We will build a culture of ongoing learning and listening, to better understand the needs of Aboriginal people, their families and communities.
Collective outcome statement
Together, we contribute to a system that recognises, understands and supports the wisdom and resilience of Aboriginal people. We recognise the impacts of colonisation and intergenerational trauma. We seek to create a system that is safe, nurturing and culturally responsive.
Aboriginal self-determination [will be] respected and upheld in the design and delivery of treatment, care and support, and Aboriginal people can choose to receive care within Aboriginal community-controlled organisations, within mainstream services or a mix of both. Irrespective of where treatment, care and support is delivered for Aboriginal people, communities and families, it is fundamental that it is safe, inclusive, respectful and responsive (Royal Commission into Victoria’s Mental Health System, Final report, Volume 3, p 143.)
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- current Victorian guidelines, policies and frameworks that guide culturally safe and responsive care for Aboriginal consumers, families, carers, supporters and communities
- the importance of self-awareness in culturally safe practice
- Australian precolonial and postcolonial history, including the Stolen Generations, and the impact of colonisation on Aboriginal health and wellbeing
- social determinants of Aboriginal health and wellbeing, including political, social and historical determinants
- Aboriginal concepts of social and emotional wellbeing, including the central importance of connectedness to emotional, physical, cultural and spiritual wellbeing
- the importance of relationships to cultural safety and cultural responsiveness, and how to work towards these objectives at an individual, community and systemic level
- Aboriginal self-determination, and that it is enshrined in state legislation and central to Closing the Gap
- preferred language, terminology and understandings of mental health informed by current Aboriginal policy directives and persons, including concepts of family and kin, and concepts of healing.
The mental health and wellbeing workforce will:
- practise cultural safety, build effective and meaningful relationships and adapt language and approaches. This will occur in line with Aboriginal guidelines, policies and frameworks that have been developed in collaboration with Aboriginal stakeholders and communities
- adapt practices to respond to the needs of Aboriginal consumers, families, carers, supporters and communities
- recognise and respond holistically to the cultural aspects of a person’s experience. This includes institutional racism, intergenerational trauma, spirituality and healing. It also includes creating a safe space for Aboriginal people to understand and make meaning from their story
- reflect on their own level of competency in supporting Aboriginal cultural safety, preventing bias and discrimination. This includes identifying improvements for ongoing development
- recognise and respond to the inherent cultural load experienced by Aboriginal members of the workforce
- respect the diverse roles and expertise of all workforces to collaborate to share the workload and provide the best care and support for consumers, families, carers and supporters.
Care, support and treatment roles
Those in care, support and treatment roles will:
- respect and seek to understand how Aboriginal consumers, families, and communities relate to their spirituality, ancestors, land, culture, community, family, kinship, mind, emotions and body. This includes social and emotional wellbeing, and recognising diversity within and between Aboriginal communities
- build self-awareness of our level of expertise and the influence of our own culture, experience, social networks and education. This will help us to respond safely and effectively to achieve the best outcomes for consumers, families, carers and supporters
- respect and seek out alternative sources of advice and guidance in the community to enhance understanding and practice
- support Aboriginal self-determination by providing care, treatment and support in line with preferences
- acknowledge and work to overcome discrimination and barriers to access for Aboriginal consumers, and their families, carers, supporters and communities
- collect and record data or information regarding Aboriginal status in line with the principle of self-identification and informed consent.
Technical or specialist roles
Those in technical or specialist roles will:
- embed Aboriginal concepts of social and emotional wellbeing and approaches to care and support into programs
- foster culturally safe and diversity-responsive ways of working
- support peers to adapt care, support and treatment to meet the needs of Aboriginal consumers, families, supporters and communities.
Leadership roles
Those in leadership roles will:
- embed Aboriginal voices and representation across the system
- strengthen Aboriginal employment in senior positions
- embed culturally safe and responsive ways of working
- recognise and support the wellbeing of Aboriginal members of the workforce
- embed active and ongoing reflective practice focused on working with Aboriginal people, families and communities
- provide meaningful opportunities for ongoing learning that promotes culturally safe and responsive care, support and treatment
- embed accountability mechanisms to ensure care, support and treatment is culturally safe and responds to the needs of Aboriginal people.
Reflective practice questions
- How does my engagement reflect Aboriginal concepts of connectedness in relation to social and emotional wellbeing?
- How do I incorporate self-determination in all interactions and engagements?
- What have I done to learn about the person, their family and community?
- Does the way I am working reflect self-awareness of my own level of expertise and positioning? Does this include learning opportunities for personal and professional growth with communities, peers and collaborators?
Care, support and treatment is culturally safe and welcoming for all people. It recognises and celebrates diversity. Culturally safe and diversity-responsive approaches extend to consumers, families, supporters and communities. These approaches acknowledge the many forms of often intersecting diversity, including diverse cultural, linguistic and faith communities, people with a disability, LGBTIQ people and people with many other backgrounds, attributes and characteristics.
Outcome statements
Consumer outcome statement
Those providing care, support, information and treatment seek to understand my culture, identity and background and how this influences my understanding of health and wellbeing. My definition of family is understood, valued and informs engagement.
Different expectations and understandings of family, family engagement, cultural expectations and views about health and wellbeing inform holistic responses. My needs and preferences are paramount.
I am supported by workforces who understand the importance of flexible access and connection to care and support. They consider how my diversity affects my needs.
I am culturally and psychologically safe when engaging in the mental health system.
Carer and family outcome statement
Our connection to the person we support is valued and understood. We are included in a way that is respectful of cultural and intersectional practices. Engagement with us responds to our understandings of health and wellbeing.
We are supported by a workforce who understand the importance of flexible access and connection to care and support. They consider how our diversity affects our needs.
We are culturally and psychologically safe when engaging in the mental health and wellbeing system. We are supported to engage meaningfully throughout care.
Workforce outcome statement
We recognise that diversity can exist in many forms among consumers, families, supporters and communities. We use an intersectional lens to understand those we work with.
We embrace culturally responsive and psychologically safe approaches throughout all aspects of care, support, information and treatment.
We practice in a non-discriminatory way. We are constantly aware of the effects of racism, colonisation and other form of discrimination on people’s daily lives.
Collective outcome statement
Together, we contribute to a system that is culturally responsive, psychologically safe, and based on the needs and preferences of consumers, families, carers and supporters. We recognise and negotiate people’s multiple perspectives and diverse lived and living experiences.
Key knowledge and skills
Whole mental health and wellbeing workforce
The mental health and wellbeing workforce understand:
- current Victorian guidelines, policies and frameworks that guide culturally responsive and psychologically safe care
- different types of diversity, including gender, culture, religion, disability, age, power, status, sexual preference and values systems
- the multiple forms of discrimination and disadvantage, including those articulated in Victorian and Commonwealth discrimination legislation
- the unique and individual ways that people from diverse communities and their families, carers and supporters relate to their own culture and community
- intersectionality, and how it influences the way people engage with the mental health and wellbeing system.
The mental health and wellbeing workforce will:
- ensure care, support and treatment is respectful and responds to the diverse backgrounds and identities of consumers and their families. This includes accepting the legitimacy of differences in realities and experiences for all consumers, carers and families
- embed cultural safety practices, language use and approaches in line with people’s needs and those of their personal supports. This includes using relevant guidelines, policies and frameworks developed in collaboration with diverse people and communities
- draw on community resources, interpreters (AUSLAN and languages other than English), and other support services to ensure clear communication and comprehension
- promote safe and sustainable engagement with personal supports, including interpreters (AUSLAN and languages other than English), carers and families
- reflect on their own level of awareness and competency in supporting cultural safety and diversity. This includes how they prevent discrimination and bias, and identifying improvements for ongoing development
- examine their own assumptions and understanding of historical and social contexts
- work to shift authority and power from systems and organisations to consumers, families, carers and supporters
- recognise and respond to the inherent cultural load experienced by diverse members of the workforce
- acknowledge the role of all workforces have in sharing the load.
Care, support and treatment roles
Those in care, support and treatment roles will:
- seek to understand how the consumer relates to their identity, culture and community, and how this might influence their needs and preferences
- consider different beliefs about health and values when shaping care, support and treatment with consumers, families, carers and supporters
- recognise and respond to the consumer’s context. This includes their experience of intergenerational trauma, marginalisation and other aspects of structural inequity
- adapt care, treatment and support to the consumer’s needs
- seek to overcome barriers to accessing by using cultural advisers and interpreters
- recognise the power dynamics that arise when working with interpreters. Work alongside interpreters in ways that support client centred outcomes.
Technical or specialist roles
Those in technical or specialist roles will:
- guide understandings and workforce capabilities in safe exploration of diversity
- guide understandings of culturally safe approaches and ways of working that respond to diversity
- support peers to adapt care, support and treatment to meet the needs of diverse consumers, families, supporters and communities
- support and guide the use of interpreters to deliver outcomes as appropriate.
Leadership roles
Those in leadership roles will:
- embed diverse voices and representation throughout services and the system
- embed culturally safe and responsive ways of working
- recognise and support the wellbeing of members of the workforce from diverse communities
- embed active and ongoing reflective practice that focuses on working in ways that are culturally safe and respond to diversity
- provide meaningful opportunities for ongoing learning that promotes culturally safe and responsive approaches to care, treatment and support
- embed accountability mechanisms to ensure care, support and treatment is culturally safe and responds to the needs of diverse individuals, carers, and families.
Reflective practice questions
- What have I done to learn about the person, their family and community?
- How have I addressed power differentials? How am I mirroring the language used by the person and family to show I am listening and curious?
- How have I used my knowledge of my own cultural background to understand assumptions I may be making in my practice?
- How have I or my organisation ensured that consumers accessing my service are able to engage in our services?
- What have I done to prepare myself to work with an interpreter?
Care, support and treatment recognises the prevalence of trauma. It uses trauma-informed approaches to empower consumers in their recovery by emphasising autonomy, collaboration and strength-based approaches. Care, support and treatment recognises that people can be traumatised through their engagement with mental health services and treatment and takes action to minimise this at every point.
Outcome statements
Consumer outcome statement
Care, support, information and treatment recognises all my experiences. It acknowledges, understands and responds to the effects of my experience of trauma with care and compassion.
Care, support, information and treatment recognises that I can be traumatised or retraumatised by the way they engage with me. This includes when they use restrictive or coercive approaches, and when my choice and control is limited.
Carer and family outcome statement
Care, treatment and support for the person we care for engages with us in ways that acknowledge, understand and respond to the effects of trauma.
Our experience of trauma, whether personal, intergenerational or vicarious, is acknowledged. We are supported and understood, alongside the person we care for.
Workforce outcome statement
We recognise that trauma can affect mental health and wellbeing. We do all we can to provide responses that respond to trauma. We seek to minimise the potential for harm, traumatisation, or retraumatisation.
We recognise the experience and impact of trauma on particular communities including but not limited to first nations, refugees, people who use alcohol and other drugs, people living with disability and LGBTIQ people.
We also acknowledge the effects of trauma, including vicarious trauma, on our wellbeing, safety and practice. We are supported in our workplace. We receive regular reflective practice supervision and ongoing professional development in trauma.
Collective outcome statement
Together, we contribute to a system that prioritises safety, trustworthiness, choice, collaboration, and empowerment. The mental health and wellbeing system minimises the potential for harm, traumatisation and retraumatisation.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- the concepts and applications of trauma-informed practice. These include trauma awareness, promoting safety, rebuilding control, focusing on strengths, promoting connection and belief in recovery
- that consumers, families, carers and supporters experience traumatic events differently
- that the effects of trauma depend on factors such as age, culture, background, social context and previous experiences of trauma, including its duration, frequency and extent
- the prevalence of trauma, including the extent to which trauma is reproduced by and within health services
- the importance of forming collaborative relationships in trauma-informed practice and care
- the importance of minimising interactions and situations that remind people of their traumatic experience and cause distress
- treatment, care and support aims to be culturally safe and responsive, including reducing discrimination and stigma that can worsen the effects of trauma
- that establishing a sense of physical and psychological safety is foundational to all engagement for both consumers and the workforce
- that early experiences of trauma shape development and can have an ongoing influence on a person’s experience of themselves, others and their environment
- that people have their own unique ways of coping with trauma. Workers should aim to understand and harness these strategies where appropriate, and minimise labelling or stigmatising negative coping behaviour.
The mental health and wellbeing workforce will:
- value the knowledge and lived experience of people who have experienced violence, trauma, and other adverse experiences
- create safe, supportive and enabling environments that minimise the risk of traumatic experiences and retraumatisation
- respond compassionately to consumers, families, carers and supporters. This includes seeking to understand the person’s experience, and the unique ways people and families cope with trauma
- maximise trustworthiness with consumers, families, carers and supporters by communicating information, processes and roles clearly and consistently
- provide accessible information, and ensure processes and care respond to the person’s gender, culture and identity
- maximise choice and control for consumers, families, carers and supporters
- collaborate with consumers, families, carers and supporters to build skills, confidence and empowerment
- identify systemic factors that make trauma worse, and advocate to overcome these barriers or find ways to mitigate their impacts.
Care, support and treatment roles
Those in care, support and treatment roles will:
- be mindful of the possibility of trauma in the lives of everyone seeking support
- apply the core principles of safety, trustworthiness, choice, collaboration and empowerment, and respond appropriately to trauma disclosure
- support trauma survivors, including people from diverse backgrounds
- minimise the risk of retraumatisation and promote healing
- promote physical and psychological safety for everyone. This includes identifying and effectively responding to current experiences of abuse and violence
- recognise the different ways people respond to trauma how this affects help-seeking and relationships
- collaborate with consumers, families, carers and supporters and affirm their strengths and resources
- focus on the whole context in which a service is provided so that the service environment and systems support safety, choice and collaboration.
Technical or specialist roles
Those in technical or specialist roles will:
- provide expert guidance and direction to support trauma-informed practices
- support peers to adopt trauma-informed ways of working
- support education and training initiatives for trauma-informed practice
- use best practice interventions and understand the importance of care coordination in promoting choice and control.
Leadership roles
Those in leadership roles will:
- embed principles of trauma-informed practice across the system, including in the design and delivery of care, support and treatment
- put in place meaningful systems to gather feedback from consumers, carers, families and supporters. Ensure that this continuously informs ongoing service review, planning and design
- prioritise staff’s physical and psychological safety when they disclose vicarious trauma or direct exposure to traumatic incidents, and access training to help you do this
- ensure there are people with lived experience of trauma working at all levels of the system, including leadership
- work in partnership with people with lived and living experience to co-design strategies, policies and targets to embed trauma-informed practice across the mental health and wellbeing system
- provide meaningful opportunities for ongoing learning on trauma-informed care, support and treatment for all staff
- embed accountability mechanisms to ensure care, support and treatment is trauma-informed.
Reflective practice questions
- How do I promote a sense of physical and psychological safety in all engagements with consumers and workers?
- How do I consider what is happening for this person (rather than what has happened to this person)?
- How do I demonstrate respect and understanding for someone’s experience, recognising that previous experience shapes our responses?
- What do the people using our services need to know in order to feel like they have choice and are in control?
- How do I ensure that our service takes a strengths-based approach to care?
- How do I communicate hope for recovery for consumers, carers, families and supporters?
Care, support and treatment recognises risk and protective factors. It uses strategies to respond to crisis and risk, including involving the person's family, carers and supporters. Services understand the impact of grief following suicide and provide support for families, carers, supporters, communities and the workforce.
Outcome statements
Consumer outcome statement
I am listened to and responded to with care and concern when I am in crisis. I feel heard.
I am supported to navigate the mental health and wellbeing system. I can access and receive collaborative care and crisis support that meets my needs in a timely way. This care supports me through my crisis safely and completely.
I am actively engaged in a process of collaborative planning and supported decision-making. I lead the development of an agreed plan that ensures my safety and wellbeing.
Carer and family outcome statement
Our concerns are heard and responded to. They inform a plan that encompasses the safety and wellbeing of everyone involved.
We are confident that the person we support is in safe hands and actively engaged in a process of supported decision-making.
We are enabled to navigate the mental health and wellbeing system and access collaborative care and crisis support at all times.
The effects of mental health crisis and suicide on families, carers and supporters is recognised and responded to.
Workforce outcome statement
We understand the unique social, economic, historical, and environmental factors that contribute to a person’s psychological distress, mental health crisis and/or suicidality. We feel confident to support the person, their family, carers and supporters to manage these risk factors in safe and minimally restrictive ways.
We recognise the effects of psychological distress and mental health crisis on the whole family and person’s support network. We support consumers, families, carers, and supporters to navigate and access collaborative care and crisis support.
Collective outcome statement
Together, we contribute to a system that recognises and responds to the unique needs of everyone affected by psychological distress, mental health crisis and/or suicide. We work together to understand the person’s context and provide support to families, carers and communities at every point of care.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- the range of life circumstances and social determinants that affect psychological distress, mental health crisis and suicidality
- early warning signs of mental health crisis and suicide risk, including burnout and vicarious trauma, as well as risk and protective factors
- that self-harm is different to suicidality, but they can coexist
- the importance of transparent and collaborative risk assessment and care planning
- the supports and services that respond effectively to psychological distress, mental health crisis and suicidality
- responsibilities and reporting obligations relevant to risk, including self-harm, suicide and safeguarding.
The mental health and wellbeing workforce will:
- incorporate messages of hope and optimism in all interactions with consumers, families, carers and supporters
- maintain current knowledge and understanding of responding to suicide risk and crises. This includes being able to identify early warning signs of mental health crisis and suicidality. It also includes escalation to appropriate supports in accordance with the preference of consumers, families, carers and supporters while managing safety
- connect consumers, families, carers and supporters to both crisis support and longer-term support
- guide access to specialist bereavement and aftercare support
- seek support to debrief and prioritise their own self-care.
Care, support and treatment roles
Those in care, support and treatment roles will:
- recognise and respond to psychological distress, mental health crisis with compassion, and in ways that maximise autonomy and choice
- use evidence-based counselling modalities and therapeutic interventions when working with consumers, families, carers and supporters
- integrate understanding of suicidality into a broader understanding of the person and their context, including strengths and challenges
- ensure that people experiencing mental health crisis are supported to access suitable and ongoing care, support and treatment according to their needs and preferences and those of their families, carers and supporters
- collaboratively assess risk and plan care with consumers, families, carers and supporters while articulating and upholding their rights
- collaboratively develop safety plans tailored to the needs and preferences of consumers, families, carers and supporters
- prevent and manage aggression, self-harm and challenging behaviours. This includes by safely engaging and connecting, conducting comprehensive risk assessments and using safe de-escalation techniques. Always ensure the least restrictive means are used
- empower consumers, families, carers and supporters to support their mental health and wellbeing by giving people evidence-informed self-management tools and resources.
Technical or specialist roles
Those in technical or specialist roles will:
- respond to or provide expert guidance to support understanding of mental health crisis, self-harm and suicide
- provide psychological and suicide distress support based on the needs of individuals
- respond to or provide expert guidance to support understanding of specialist bereavement and aftercare support
- respond to or provide expert guidance to support understanding of critical incident response and debriefing at the individual or community level
- recognise when legal and ethical obligations may apply. Engage the assistance of senior staff and other professionals to implement care, support and treatment
- undertake or contribute to dedicated research into mental crisis, suicide and self-harm.
Leadership roles
Those in leadership roles will:
- embed safe and ethical approaches to crisis and suicide response
- foster cultures of transparency and support open discussions around risk and safety planning
- foster cultures that support safe and positive risk-taking, promoting consumer choice and agency, balancing workforce wellbeing and safety
- provide safe and supported working environments to minimise the risk of aggression, self-harm and other challenging behaviours
- ensure there are escalation processes in place to address issues of risk
- embed regular supervision practices, debriefing and supports for staff
- provide expert guidance and direction relating to fulfilling legal and ethical obligations.
Reflective practice questions
- How do I actively engage the person in options related to what they are experiencing?
- How do I support the person to feel they have power and control?
- How do I pick up on life protectors and promoters and use these in my engagements?
Care, support and treatment recognises that people experiencing psychological distress or mental illness often have intersecting needs and preferences. Services, teams and practitioners recognise the prevalence of co-occurring substance use and addiction among mental health consumers. They ensure substance use and addiction treatment is integrated with support for the person’s other mental health needs.
Outcome statements
Consumer outcome statement
I experience integrated responses to both my mental health and substance use concerns. This includes connection to services and supports that respond to both my mental health and substance use concerns.
I feel respected, hopeful, and empowered to address these related but distinct needs.
Carer and family outcome statement
We have the information and strategies we need to play our important role in the care and treatment planning for the person we support. We feel valued, supported, included and hopeful about the future.
Workforce outcome statement
We recognise the intersectional and related nature of trauma on mental health and substance use, gambling and other addictive behaviours. We provide integrated treatment that responds to co-occurring mental health and substance use, gambling and addictive behaviours. We acknowledge that harm reduction is an effective evidence-based approach to substance use.
Collective outcome statement
Together, we contribute to a system that effectively provides an integrated treatment, care and support response to people experiencing both mental health and substance use, gambling, or addiction needs.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- that substance use, gambling and other addictive behaviours commonly occur among people with mental health needs
- the effects of compounded stigma and discrimination associated with co-occurring mental health needs and substance use, gambling and other addiction behaviours. These include barriers to accessing quality care, support and treatment
- the risks, harms and unwanted outcomes associated with experiencing co-occurring mental health needs and substance use, gambling and other addictive behaviours
- that integrated care can lead to improved outcomes for people with co-occurring needs
- that people who receive siloed or non-integrated care for co-occurring needs are at risk of harm
- that people may be at different stages of change in relation to their mental health needs and any co-occurring substance use, gambling or other addictive behaviours
- local pathways to access secondary consultation for people experiencing co-occurring mental health and substance use, gambling, or other addictive behaviours
- the effects of different substances and severities of substance use issues on a person’s mental health
- what constitutes integrated treatment (as distinct from sequential or parallel treatment) and local approaches to providing or facilitating integrated treatment, care and support.
The mental health and wellbeing workforce will:
- actively welcome, engage with and meaningfully assist people to receive integrated care, treatment and support when they experience substance use, gambling and other addictive behaviours
- collaborate with people who have lived experience of co-occurring mental health and substance use, gambling and other addictive behaviours to improve the effectiveness of integrated care
- recognise the diverse care, support and treatment needs and preferences of people presenting with co-occurring mental health and substance use, gambling and other addictive behaviours
- be skilled in working motivationally and in developing helpful conversations with people co-occurring substance use, gambling or other addictive behaviours.
Care, support and treatment roles
Those in care support and treatment roles will:
- understand the possible effects of different substances, and the nature and extent of substance use, on a person’s mental health
- understand how substance use, gambling and other addictive behaviours may be a way of coping with mental health difficulties, and also contribute to those difficulties
- screen people who present for mental health care, support and treatment for co-occurring substance use, gambling and other addictive behaviours
- collaboratively develop individualised treatment plans with people, their families, carers and supporters that address co-occurring needs according to their preferences
- deliver tailored responses from brief to more intensive treatment approaches for people, depending on the severity and risks in their presenting needs
- work with people around their experiences of stigma and discrimination
- recognise and respond to symptoms of withdrawal from a range of substances. Know when and how to seek support and secondary consultation for management of withdrawal
- assess and respond to the information and support needs of families, carers and supporters
- seek and provide secondary consultations, including documentation, acting on advice and providing follow up.
Technical or specialist roles
Those in technical or specialist roles will:
- provide secondary consultation to mental health and wellbeing and alcohol and other drug practitioners and clinicians across both sectors
- support education and training initiatives for mental health and alcohol and other drug practitioners and clinicians
- provide complexity-focused clinical supervision to mental health and alcohol and other drug practitioners and clinicians
- undertake or contribute to dedicated research into co-occurring mental health needs and substance use, gambling and addictive behaviours
- develop and facilitate the use of tools and resources to recognise and respond to the needs of people experiencing mental health needs and substance use, gambling, or other addictive behaviours
Those in leadership roles will:
- use co-occurring prevalence data in all agency and systemic quality improvement activities and when allocating resources
- monitor and address access to and quality of integrated treatment for people with mental health and substance use, gambling and addictions needs
- draw on the mental health and alcohol and other drug workforces’ expertise to drive service and system improvements and effective outcomes
- actively promote and implement strategies and quality improvement activities to eliminate stigma related to substance use, gambling and other addictive behaviours
- develop relationships, collaboration and accessible treatment pathways with other services and sectors
- ensure that the service or system has the right practitioners and clinicians to provide integrated care
- advocate for integrated care approaches using reports, articles in professional journals, and media releases.
Reflective practice questions
- What are my beliefs about people with co-occurring mental health and substance use, gambling, or addiction needs?
- How can I assist a person who self-stigmatises about their experience of co-occurring needs?
- What do I understand by the term mutually influencing/bi-directional when it comes to working with people with co-occurring mental health and substance use issues?
- When working with people, what personal and professional strategies do I draw on to maintain hope and optimism?
- What do I do to reduce stigma and discrimination against people with substance use and addiction at work and in my community?
Services, teams and practitioners recognise the prevalence of family violence across the social spectrum. All care, support and treatment adopts a rights-based approach that prioritises safety, agency and empowerment through cross-sector and cross-discipline collaboration and teamwork.[1]
Outcome statements
Consumer outcome statement
I experience integrated responses to both my mental health and family violence concerns. This includes connection to services and supports that respond to my needs.
I am supported and equipped with the knowledge and skills that inform and shape healthy, safe, equal and respectful relationships.
I feel safe, hopeful and empowered to address these related needs.
Carer and family outcome statement
We are given a safe space to discuss our experiences in confidence on initial contact. We are given further opportunities throughout care.
We are supported and equipped with the knowledge and skills that inform and shape healthy, safe, equal and respectful relationships.
People at risk of witnessing or experiencing family violence are identified early and provided with quick and effective interventions. This includes children and young people.
Workforce outcome statement
We recognise mental health and family violence issues may be related. We view integrated treatment and care for both needs as part of effective practice.
We understand that family violence does not always mean physical violence. Our awareness of family violence includes physical, sexual, psychological, emotional and spiritual violence, as well as financial and economic abuse and control.
We understand the serious risk factors that significantly increase the risk to victim survivors (adults and children). We use structured professional judgement to determine the level of risk and inform risk management responses. We understand our responsibilities to undertake risk assessment and management, including information sharing and working collaboratively.
We work collaboratively with family violence, child wellbeing and other information sharing entities and risk assessment entities to reduce barriers to care and support.
Collective outcome statement
Together, we contribute to a system that effectively identifies and responds to people experiencing both mental health and family violence concerns.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- that family violence occurs when a perpetrator exercises power and control over another person. This involves coercive and abusive behaviours designed to intimidate, humiliate, undermine and isolate. These behaviours can include physical and sexual abuse, as well as psychological, emotional, cultural, spiritual, social, technological and financial abuse
- the broader definition of family violence for Aboriginal communities, which includes family violence within extended families, kinship networks and communities. It extends to one-on-one fighting, abuse of Aboriginal community workers, and self-harm, injury and suicide
- that people who use violence may use their own mental health difficulties as an excuse or justification for violent or coercive behaviours
- how abuse and violence contribute to, or cause, the person’s mental health difficulties
- that people who use violence may use the victim survivor’s mental health as a tactic of coercive control to, for example, undermine, discredit, or isolate them from services and support workers
- when the person using violence makes suicide threats, this heightens the risk of homicide or serious harm to victim survivors
- the range and patterns of behaviours that constitute family violence, including warning signs and risk indicators across the lifespan
- how to apply an intersectional lens to understand a person’s multilayered identity, life experience and experience of inequality and oppression, as well as the intersection between family violence and mental health
- their professional obligations under the Family Violence Multi-Agency Risk Assessment and Management Framework (MARAM) in accordance with their role
- family violence legislation, policies and plans relevant to their role. This includes their organisation’s requirements relating to risk assessments and family violence responses
- mandatory reporting requirements under relevant legislation and standards regarding children and young people who are victim survivors of family violence
- information sharing laws and regulations, including when risk indicates that information sharing is required despite privacy and consent concerns
- that women with mental health concerns can be more at risk of family violence due to higher levels of vulnerability
- that a consumer with a mental health issue can also be a victim or perpetrator of family violence.
The mental health and wellbeing workforce will:
- understand that victim survivors may be reluctant to engage with mental health services due to previous experiences of discrimination, fear of authorities, fear of repercussion and other barriers to help-seeking
- provide information to consumers, families, carers and supporters to assist them in understanding the support available and navigate barriers to assistance
- recognise a need for assessment of risk in relation to family violence, and follows appropriate responses in line with MARAM
- make reports to relevant authorities where assessments indicate significant risk of harm to children, young people and vulnerable people
- monitor, assess, document and report risks or threats to their own safety according to relevant policies and procedures
- ensure organisational support if the person using violence makes vexatious complaints about frontline workers or their supervisors.
Care, support and treatment roles
Those in care, support and treatment roles will:
- respect the right to confidentiality and privacy, while also working with the limitations in regard to confidentiality, risk and safety (including risk to children)
- recognise the link between mental health and family violence, including family violence as a trigger for mental illness or affecting people’s recovery from mental illness
- recognise that mental health issues for victim survivors (adults and children) may be symptoms of abuse that are directly related to coercive control
- recognise how family violence can present. Seek information required to assess whether consumers, families, carers and supporters are at risk of family violence or of witnessing this violence
- understand the cumulative and traumatic effects of family violence and its impact on mental health and wellbeing
- respect the decisions victim survivors make to manage their own safety. Support them to regain control and express their autonomy, agency and expertise in decision-making
- not make the person using violence the decision-maker, primary carer or guardian of the victim survivor
- understand that when a person accesses support or services, they may be at an increased risk of serious harm or death, which may influence their mental health and wellbeing
- understand that engaging with perpetrators around their use of violence may result in increased risk to victim survivors. Ensure mental health support and safety plans are in place
- maintain confidentiality of records and ensure the person using violence cannot access them, including in the justice context
- place responsibility for the violence on the perpetrator and never on victim survivors of family violence
- make contact with appropriate services to facilitate warm referrals, where consumer consent has been provided
- actively avoid collusion with perpetrators, recognising and rejecting attempts to minimise or deny their use of violence
- refer perpetrators to appropriate specialist services following identification or disclosure of perpetration of family violence
- work within the extent and limitations of their role regarding engagement, risk identification, preliminary assessment and referral
- seek specialist family violence support and guidance where needed.
Technical or specialist roles
Those in technical or specialist roles will:
- guide development, implementation and monitoring of safety plans, case management plans, and understandings of family violence in the context of mental health care, support and treatment
- provide secondary consultation to enhance family violence responses, including understanding and recognising the tactics of coercion, power and control that perpetrators use
- help victim survivors navigate the service system and advocate for them so as to minimise gaps in service responses
- conduct preliminary risk assessments as required by their role, following identification or disclosure of family violence, and in consultation with specialist family violence services
- address the risk management of the person using violence with the appropriate organisations. Share information and ongoing updates of the risk management plan.
Leadership roles
Those in leadership roles will:
- draw on the expertise of the mental health and family violence workforce’s to drive service and system improvements and effective outcomes
- drive an organisational culture that understands and responds to family violence
- develop collaborative relationships and accessible pathways to effectively support people experiencing family violence, including with local family violence services
- make modifications to operations to ensure the ongoing support and safety of victim survivors, in consultation with specialist family violence services
- in conjunction with specialist providers, lead ongoing development, implementation and monitoring of safety plans, case management plans and understandings of family violence.
Reflective practice questions
- How have I considered and assessed family violence in my decision-making?
- How could I seek further information or a secondary consultation to assist me to identify and respond to family violence in my work?
- What are the serious risk factors that may lead to the increased risk of harm to the victim survivor and how do I consider these in my practice approach?
- How have I adjusted my practice when I work with children and young people, or when children and young people are involved?
- How have I adjusted my practice when I work with various communities, including Aboriginal people experiencing violence, LGBTIQ communities and older people experiencing violence?
- How can I use an intersectional lens in my practice? How do I consider barriers to support that people may face because of their individual experiences, as well as barriers due to the intersection between family violence and mental illness?
- How do I understand the need for multidisciplinary collaboration and how do I implement this in my practice?
[1] State Government of Victoria 2017, Responding to Family Violence Capability Frameworks.
Care, support and treatment recognises that the consumer lives within the context of family and other relationships. It involves family and other supportive people through practice models that deliver benefits for the consumer and their families, carers and supporters.
Outcome statements
Consumer outcome statement
My family, carers and supporters are meaningfully involved in my care, support and treatment. This happens in ways that respect my individual preferences and context, acknowledging that this may change over time.
There is respect for and deep understanding that I have unique and sometimes complex relationships with family, carers and supporters.
I am compassionately listened to about the relationships that support me.
Carer and family outcome statement
The impact of mental health challenges on the whole family system is recognised, understood, and supported. Our family members who are vulnerable, including children, young people and ageing family members, are given special consideration.
We are meaningfully and actively involved in ways that visibly respect our relationships, roles, contribution and context.
Care, support and treatment recognises, draws on and enhances strengths and protective factors, and minimises harm to families, carers and supporters.
We understand our role in supporting recovery. We are supported to understand and make choices about the ways in which we provide support and care.
Our needs as family members, carers and supporters are recognised and responded to in ways that support our own health and wellbeing.
Workforce outcome statement
We understand that connections are a vital component of holistic and wellbeing-oriented care. We understand that a person’s relational context and social supports can enhance their mental health and wellbeing.
We support people to establish or develop meaningful relationships and connections in their communities, in line with their preferences.
We assist families, carers, and supporters to access supports for themselves, including children and young people.
Collective outcome statement
Together, we contribute to a system that acknowledges that family, carers and supporters play a key role in supporting consumers. The system recognises and responds families and carers in their own right. The impact of mental health challenges on the whole family system is recognised, understood, and supported.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- consumers’ interpersonal relationships are critical to their mental health recovery
- family and supporters are likely to be affected by the person’s mental health difficulties, even if they are not in an ongoing caring role
- people in ongoing caring roles experience significant emotional, physical, financial and social impacts. This increases the risk they will develop their own mental health difficulties. At the same time, they may also derive meaning and a sense of purpose from their caring role
- families, carers and supporters have diverse needs. These needs vary according to factors such as the nature of their relationship with the person (for example, dependent children or older parents), the nature of the mental illness, and broader factors such as cultural background, gender and social class
- consumers are not passive recipients of care. There are reciprocal aspects of care relationships
- including family, carers and supporters in care can improve outcomes for consumers, families, carers and supporters. In most circumstances, practitioners can create trusting relationship with the consumer and constructively include family and supporters in treatment and care
- the family environment can be both supportive and also a context in which violence and abuse occurs for consumers and for their family members
- where families, carers or supporters cannot be actively included in a person’s care, they should be given information and access to family and carer-specific services, supports and resources
- the policies and practice guidelines about inclusive family practice, and their application within their service context
- there is legislation that describes the obligations of services to include family, carers and supporters
- there are provisions that govern the sharing of information about consumers with family, carers and supporters.
The mental health and wellbeing workforce will:
- explore the person’s family and social network with them and identify who is important for their care and support
- support people to use and improve existing relationships with family and other supporters
- ask who the person wants to be included in their treatment and care and how this can occur
- reach out to families, carers and supporters the person identifies as important in their life
- adopt a needs-based approach to respond to families, carers and supporters that recognises both their caring role and the effect of the person’s mental health difficulties on them
- provide emotional support to families, carers and supporters that recognises their experience of the person’s mental health difficulties. Understand that the process of accessing and receiving treatment may also be distressing for them
- provide families, carers and supporters with information about the person’s mental health difficulties, having regard to the person’s wishes and preferences and legislative requirements
- acknowledge the effect of the consumers mental health difficulties on other family members, help them navigate the mental health system and provide information about family and carer-specific services
- use person-centred and wellbeing-oriented language and behaviour
- promote positive health and wellbeing for carers, families and supporters
- acknowledge the substantial contribution families, carers and supporters make within the mental health system.
Care, support and treatment roles
Those in care, support and treatment roles will:
- identify family members, carers and supporters (including potentially vulnerable members such as dependent children, younger and older carers) at first contact with the service
- collect, review and maintain family members’ and carers’ contact information
- give families and carers information and support at first contact and as their needs change over time
- use a relational recovery approach to practice and recognise that families, carers and supporters will have their own recovery journey
- understand, enable and support the role of family, carers and supporters in supporting a person’s wellbeing
- balance the person’s needs and preferences with those of families, carers and supporters
- be aware of family violence and, if appropriate to their role, respond in a way that increases safety for consumers, family members, carers and supporters
- promote the needs of family, carers, and supporters. Enable them to identify, discuss and access support for their own needs
- identify the needs of families, carers and supporters that may be outside the scope of their role or capability. Know how to access specialist consultation and or referral
- be aware of circumstances in which the consumer and their family, carers and supporters may benefit from specialised family interventions
- refer carers to organisations that can support them to advocate for the consumer or their own needs when this is required
- identify support needs and make appropriate referrals.
Technical or specialist roles
Those in technical or specialist roles will:
- provide expert guidance and direction to support practices that include families, carers and supporters
- provide support for peers to adopt ways of working that include families, carers and supporters
- support consumers, carers and families to become peer supporters or family advocates
- be aware of the range of family-based practices and interventions.
Leadership roles
Those in leadership roles will:
- provide evidence-based interventions that improve outcomes for family members and consumers
- advocate within their service to improve whole-of-system responses for families, carers and supporters
- embed principles of family, carer and supporter-inclusive practice across the system, including in the design and delivery of care, support and treatment
- embed carer, family and supporter representation across all levels of the system, including governance and leadership
- provide meaningful opportunities for ongoing learning that promote carer, family and supporter-inclusive care, support and treatment
- embed accountability mechanisms to ensure care, support and treatment includes and responds to the needs and preferences of families, carers and supporters, as well as consumers.
Reflective practice questions
- What is my experience of ‘family’ in my own life? How does this affect my attitudes towards including families in care?
- How do I make sense of the role of families and supporters? How does this align with or contradict contemporary approaches to family-inclusive practice?
- How comfortable am I meeting with families? What constraints (personal, professional and organisational) do I have when engaging with families? How can I address at least one of these constraints?
- Reflecting on my current work, how do I involve families, carers and supporters in the work I do with consumers? Do I routinely ask consumers about their family and support networks and explore the possibility of including them in care?
- What formal learning and knowledge and practice experience do I have that might be valuable to families?
Care, support and treatment undertakes collaborative planning, decision-making and action. It does this by sensitively exploring and actively engaging with the person and their family, carers and supporters to understand people’s differing needs.
Outcome statements
Consumer outcome statement
I am positioned as an expert in my lived and living experience and recovery journey. I understand and choose the options available to me for care, support and treatment.
I can safely voice my preferences, needs and concerns. These are treated with compassion, respect, and timely and appropriate action.
Carer and family outcome statement
Our role in caring for those we support is valued and respected. It informs the assessment process.
Our knowledge, experience, preferences, resources and strengths inform a holistic understanding of the person we care for. We collaborate in their care planning.
Our own wellbeing is considered and supported throughout the assessment and treatment planning process.
Workforce outcome statement
We work in partnership with consumers, families, carers and supporters to understand and plan options for care, support information and treatment.
We understand and respond to the experiences and preferences of consumers, families, carers and supporters. We equally value their expertise equally.
We understand the need to work with consumers where they are at now and where they would like to be.
Collective outcome statement
Together, we contribute to a system that supports people by understanding individual, family, carer and supporter needs, from their perspective. We provide options for care and tools to assist in decision-making.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- the value of holistic assessment, factoring in information from a range of sources, including families, carers and supporters
- a range of assessment options, including age-specific, discipline-specific and culturally relevant assessments commensurate with role and experience
- the value and need of point-in-time and ongoing assessment as a central part of mental health practice
- how the person’s physical, financial and support resources affect care and treatment decisions
- local services and sources of care, support and treatment, including crisis response and supports
- how intersecting factors affect mental health, including environmental, biological, and contextual factors. This includes pre-existing mental health issues such as substance use, neurodevelopmental issues or trauma.
The mental health and wellbeing workforce will:
- respond to people’s needs and preferences. It will adapt practices based on age, developmental stage and unique personal and community context
- practice supported decision-making by working with and enabling consumers to make choices about their treatment. This includes planning and decision-making that is oriented towards their goals
- promote positive and healing interactions at all points of contact
- recognise when to seek support or assistance from senior professionals or peers, and refer on when needed
- support a positive experience for consumers, carers and families. This includes appropriate escalation pathways with respect to safety planning and risk assessment.
Care, support and treatment roles
Those in care, support and treatment roles will:
- embed respect, dignity and hope into assessment and care planning
- incorporate biopsychosocial understandings of mental health and wellbeing into assessment and care planning
- explore relevant care options and their possible contributions to a person’s wellbeing and recovery. These include biological and pharmacological treatments, psychological and psychotherapeutic approaches, psychosocial rehabilitation and support, physical health care, physical activity and exercise, alcohol and drug treatment and counselling, traditional healing in different cultures and alternative and complementary treatments
- understand the relationship between a person’s early life experiences, current circumstances and broader social context
- understand the relationship between physical health, mental health, disability and coexisting conditions, including drug and alcohol use. Collaborate to address these needs simultaneously
- assess and support consumers’ physical health needs. This can include support to quit or reduce smoking, improve metabolic health (weight and diet, physical activity and fitness), sexual and reproductive health and blood-borne viruses, medicine optimisation and oral health
- undertake crisis assessments or mental state assessments as necessary and in line with practice principles and responsibilities
- support integrated ways of working with other individuals, teams and organisations to address co-occurring issues, including but not limited to substance use and addiction, homelessness and family violence
- engage diverse expertise to support the choices and goals of consumers, families, carers and supporters
- recognise and celebrate strengths and existing resources, including carers, family, and supporters.
Technical or specialist roles
Those in technical or specialist roles will:
- deliver or provide expert guidance and direction on holistic assessment and care planning
- deliver or provide expert guidance and direction on approaches to collaboration
- provide secondary consultation, giving specialist advice and support to other members of the workforce
- support reflective practice and problem-solving to embed collaboration in all aspects of assessment and care planning
- support peers to embed compassion and collaboration into care, support and treatment.
Leadership roles
Those in leadership roles will:
- embed collaborative ways of working in all elements of assessment and care planning
- model collaborative leadership, promoting the value of diverse expertise, including lived experience
- provide meaningful opportunities for ongoing learning that promotes holistic assessment and collaborative care planning
- provide meaningful opportunities for collaboration with a diverse range of services and expertise, including lived experience expertise and non-mental health services.
Reflective practice questions
- How have I used a variety of information sources to conduct my assessment?
- Whose information am I privileging and why? Are there any perspectives that I have not heard or that I have dismissed? Why?
- Have I reflected on any assumptions or influencing factors that may affect my thinking?
Care, support and treatment uses tailored approaches with demonstrated effectiveness. It is delivered with empathy and compassion.
Outcome statements
Consumer outcome statement
I am heard, understood and responded to with empathy, respect and compassion at all times. I lead the direction of my care, support, information and treatment. This includes how my family, carers and supporters can be involved if I choose.
My safety and autonomy are prioritised at all times. This is done through the least restrictive means and high-quality, evidence-informed practice.
Carer and family outcome statement
We are given the time and respect to ensure we are genuinely heard.
Our role is valued as key partners in reducing relapse and aiding recovery. We are validated and treated with compassion for our own experience of very challenging times.
We are actively engaged in a process of collaborative and supportive discharge planning. Our preferences and capability to contribute to ongoing care are considered.
We are treated with empathy, respect and compassion at all times.
Workforce outcome statement
We work in partnership with consumers, carers, families and supporters to deliver compassionate care, support, information and treatment.
We are supported to practise in a compassionate way. This is valued and enabled through systems and processes.
We value, respect and uphold the unique experiences, hopes, needs, autonomy and preferences of everyone we support.
We understand the importance of collaborative and supportive discharge planning.
We treat everyone with dignity, respect and compassion. We work with consumers/services users where they are.
Collective outcome statement
Together, we contribute to a system that compassionately supports everyone to live a full and meaningful life.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- the importance of ensuring that all care, support and treatment is integrated and collaborative, and responds to the person’s needs, including for social and economic supports
- the importance of respectful and trusting relationships, and the implications of failing to centre respect and trust
- the social determinants of health and wellbeing, including political, social and historical determinants
- the personal nature of wellbeing and recovery. This includes considering factors such as social, cultural and economic context, past experiences and presenting issues
- the importance of carers, families, supporters and communities to mental health wellbeing and recovery.
The mental health and wellbeing workforce will:
- embrace compassionate and empathetic ways of working that focus on strengths and wellbeing
- employ psychologically safe practices. This includes language use and engagement that is in line with current practice guidelines, policies and frameworks developed in collaboration with consumers, families, carers and supporters
- respond to the range of needs and preferences of consumers, families, carers and supporters. This includes adapting practices based on age, developmental stage and unique personal and community context
- recognise when to seek supervision, personal support or assistance from other professionals or peers
- follow processes and protocols to support positive experiences for consumers, carers and families. This includes appropriate escalation pathways for safety planning and risk assessment.
Care, support and treatment roles
Those in care, support and treatment roles will:
- embed respect, dignity and hope into care, support and treatment
- develop authentic and professional relationships with consumers, families, carers and supporters while maintaining safe and professional boundaries
- demonstrate respect for the lived experience of consumers, carers and families. This includes through active listening, checking understanding and refraining from judgement and assumptions
- draw on a range of approaches that support wellbeing and recovery, including those developed by people with lived experience of mental health issues
- practise supported decision-making by working with and enabling consumers to make choices about their treatment. This includes planning and decision-making that is oriented towards their goals
- work with consumers, families, carers and supporters to collaboratively shape care, support and treatment, acknowledging and exploring potential risks and benefits
- engage diverse expertise to support the choices and goals of consumers, families, carers and supporters
- adapt care, support and treatment to meet the evolving needs and preferences of consumers, families, carers and supporters
- apply person-centred principles to respond compassionately to consumers, families, carers and supporters
- consider the therapeutic appropriateness of self-disclosure based on the needs of the person seeking care, and use it selectively when appropriate
- monitor care, support and treatment for possible side effects, risks and efficacy, in collaboration with consumers, families, carers and supporters
- engage diverse expertise to support the choices and goals of consumers, families, carers and supporters
- recognise and celebrate progress, wellbeing and recovery.
Technical or specialist roles
Those in technical or specialist roles will:
- provide technical or specialist mental health care, support and treatment
- provide expert guidance or direction to support practice that focuses on strengths and wellbeing
- support peers to adopt strengths-based and wellbeing-oriented ways of working
- provide secondary consultation, including specialist advice and support to other members of the workforce
- support people with relevant interest and capabilities to become advocates or peer workers
Leadership roles
Those in leadership roles:
- model compassionate leadership to promote the values of curiosity, collaboration and care
- drive workplace cultures that respond to the needs of consumers, families, carers and supporters and that are open to new ways of working that enhance wellbeing and recovery
- enable and support the practice of compassionate care and build workplace cultures that value quality care, support and treatment
- embed lived experience in the design and delivery of care, support and treatment and at all levels of the system, including leadership
- provide meaningful opportunities for ongoing learning that promotes compassionate care, support and treatment
- embed accountability mechanisms to ensure care, support and treatment is compassionate, collaborative and responds to needs and preferences of consumers, families, carers and supporters
Reflective practice questions
- What have I done to build rapport, and ensure that those with whom I am engaging feel respected, heard and safe?
- What is and is not working when building a therapeutic relationship with this consumer, family, carer or supporter?
- Am I listening to what the consumer values? Do I look for ways to incorporate these values and ways of thinking into treatment, care and support?
- How do I adapt my approach as the needs and preferences of the consumer change?
- Have I sought out opportunities for supported reflection to increase compassion in my practice?
Care, support and treatment facilitates wellbeing and resilience through promoting prevention, early intervention and help-seeking. Engagement empowers individuals, families and communities to enhance their strengths. It also provides them with resources to support personal health and wellbeing goals.
Outcome statements
Consumer outcome statement
I am empowered to access information and supports that enhance my understanding of my mental health and wellbeing. This enables me to be physically and mentally healthy and well in my day-to-day life.
I am enabled to practise self-care and build my own resilience. I am encouraged and assisted to access care and support whenever I am in need, not just when I am in crisis.
I am enabled to make informed choices about my own mental health and wellbeing and be actively involved in decision-making about the type of health and mental health care I receive.
Carer and family outcome statement
Our mental health and wellbeing as a whole family, carer and supporter network is considered (inclusive of the consumer) and services respond proactively to us, maintaining and promoting our mental health and wellbeing.
We have access to information and supports that enhance our understanding of mental health and wellbeing.
We are supported to access care and support whenever we too are in need.
Workforce outcome statement
We work to enhance positive mental health and wellbeing for all.
We work to destigmatise mental illness and suicide and promote access to a range of preventive or responsive mental health and wellbeing supports.
We understand health inequity and work in ways that seek to address inequities. We will provide information and education to consumers so they can make informed decisions.
Collective outcome statement
Together, we contribute to a system that proactively promotes positive mental health and wellbeing through promotion, prevention and early intervention approaches. These approaches empower consumers, carers, families and supporters to prioritise their mental health and wellbeing and seek support at any stage of life.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- the importance of mental health promotion efforts to prevent mental health conditions, support mental health literacy, help-giving, and help-seeking for mental illness, psychological distress and suicidal ideation
- the social determinants of mental health. These include individual, familial, social, cultural and economic risk and protective factors, and the impacts they have on mental health and wellbeing
- the impact of stigma and discrimination on mental health and wellbeing
- the influence of culture on mental health and wellbeing, and the principles of human rights and health equity
- approaches to mental health promotion and prevention that reduce incidence, prevalence and recurrence of mental illness and psychological distress
- the programs, public policies, service systems and supports that are needed and available to facilitate promotion, prevention, help-seeking and early intervention.
The mental health and wellbeing workforce will:
- offer information that support consumers, families, carers and supporters to adopt self-care strategies or connect them with services that promote their wellbeing
- support consumers, families, carers and supporters to develop and sustain their relationships, support networks and community connections
- raise awareness of mental health and wellbeing at an individual, community and population level
- work to reduce stigma and discrimination in all its forms and promote help-giving and help-seeking
- support consumers, families, carers and supporters to find and access mental health and wellbeing supports, no matter when, where or how they present in need of care
- advocate for action to address the social, cultural, economic and systemic determinants of mental health
- actively contribute to increased accessibility and improved outcomes for Victorians, with an emphasis on achieving health equity
- prioritise their own personal wellbeing, while working to support the mental health and wellbeing of consumers, families, carers and supporters.
Care, support and treatment roles
Those in care, support and treatment roles will:
- embed principles of wellbeing, prevention and early intervention into care, support and treatment
- build their own and consumers’, families’, carers’ and supporters’ understanding of the risk and protective factors that influence mental health and wellbeing
- understand, champion and apply wellbeing and preventive approaches. These approaches include those developed by people with lived experience of mental health issues
- promote opportunities to improve mental health and wellbeing through holistic means. For example, this includes exercise, nutrition, sleep hygiene, spirituality and stress management
- provide opportunities for consumers, families, carers and supporters to build and maintain their social supports and community connections
- implement strategies to prevent the onset of psychological distress or mental illness
- build mental health literacy and equip people to recognise and deal with the signs and symptoms of psychological distress or mental illness as soon as possible
- build confidence in accessing care, support and treatment
- understand, champion and apply a range of early intervention approaches, including those developed by people with lived experience of mental health issues
- seek to minimise psychological distress at an early stage and prevent its recurrence or progression
- build insight into the importance of proactive decision-making and care planning
- provide information and choice, and facilitate access to help and support for consumers, families, carers and supporters
- promote the importance of support and wellbeing from, and for, families, carers and supporters
- support peers to adapt care, support and treatment to incorporate health promotion, prevention, and early intervention responses.
Technical or specialist roles
Those in technical or specialist roles will:
- deliver or provide expert guidance and direction to support understanding of, and engagement in, mental health promotion initiatives
- deliver or provide expert guidance and direction to support understanding of wellbeing, prevention and early intervention
- deliver or provide expert guidance and direction on approaches to coordinated care
- build multidisciplinary teams to support consumers, families, carers and supporters
- deliver or provide expert guidance and direction to support understanding of service system and referral pathways.
Leadership roles
Those in leadership roles will:
- identify causal and risk factors for health and wellbeing trends, evaluating impact and developing local and population level solutions
- ensure mental health and wellbeing is central to services policies and processes
- develop effective partnerships with key stakeholders, gatekeepers and target group representatives. This will ensure mental health promotion activities meet the needs of the community, including diverse communities
- advocate for prevention and early intervention using reports, journal articles and media releases
- embed active and ongoing reflective practice that focuses on wellbeing, prevention and early intervention
- embed active and ongoing reflective practice that focuses on facilitating help-seeking and fostering self-care
- provide meaningful opportunities for ongoing learning that promotes wellbeing, prevention and early intervention.
Reflective practice questions
- How do I apply an understanding of the social determinants of mental health and wellbeing to my work?
- How do I include a strong focus on wellbeing promotion, and self-care into my practice?
- How am I incorporating prevention and early intervention in my work and my workplace?
- How can I raise awareness of mental health at a range of levels to combat stigma and discrimination?
- How am I supporting consumers, carers, families, and supporters to understand, navigate and access mental health and wellbeing supports?
Care, support and treatment helps people to navigate the mental health and wellbeing system. This includes providing service and referral options and pathways that enable continuity of care and individual choice.
Outcome statements
Consumer outcome statement
I am informed about the various people and agencies that can be involved in my care, support, and treatment, and where and how I can get more information.
Supported decision-making helps me make choices about which people and agencies I wish to be involved and for what.
I understand my rights and what information will and will not be shared with services.
The people providing my care have collaborated within and across services. This has ensured services holistically support my improved mental health and wellbeing.
Carer and family outcome statement
We understand the pathways within the system and can navigate it in a straightforward manner.
We are clear about the roles of all involved. We know who to call and when, and they will know our circumstances. We know our rights and what information will and will not be shared with services.
There is no wrong door for access to service for the person we support and ourselves.
Workforce outcome statement
We respect and value the distinct expertise, knowledge values and diverse experience that exists across the mental health and wellbeing workforces. We use this to ensure consumers, families, carers and supporters can navigate the system and have continuity of care. We appreciate the strengths and values of working within a multidisciplinary team. We embrace the diversity that exists within the workforce, including lived experience and discipline-specific expertise.
We understand our obligations in relation to privacy and confidentiality. We know when and how to respectfully share information within a consumer’s network.
We commit to working collaboratively to facilitate positive mental health and wellbeing outcomes for consumers, families, carers and supporters.
Collective outcome statement
Together, we contribute to a system that enhances quality service provision through effective working relationships to ensure people receive integrated and coordinated care, support and treatment.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- the service landscape, including how to access primary care and prevention, assessment and support, crisis response and aftercare
- that collaboration across systems should include the full range of related services. This includes health, social services, education and criminal justice systems
- system-level barriers that prevent people from accessing and engaging with the service system
- the value that diverse workforce experience and expertise might have for consumers, families, carers and supporters
- current information on partner agencies such as intake criteria, approximate waiting times and required processes/forms for referral
- the significant impact that continuity of care has on experiences and outcomes
- responsibilities associated with informed consent, privacy and confidentiality
- responsibilities related to data collection and storage, relevant information management and sharing, as well as systems and protocols.
The mental health and wellbeing workforce will:
- support consumers, families, carers and supporters to navigate the service system and find supports in a timely and responsive way
- work in collaboration with consumers, families, carers and supporters, and the wider workforce to mitigate systemic barriers to health and wellbeing
- advocate on behalf of consumers, families, carers and supporters with other individuals, teams and organisations
- demonstrate flexible and inclusive practice that values and acknowledges all levels of expertise
- communicate in ways that promotes mutual respect and fosters a shared understanding
- model respectful language and collaborative engagement, recognising that diversity may exist within and between professions in relation to their practice
Care, support and treatment roles
Those in care, support and treatment roles will:
- demonstrate a current local knowledge of other service providers and their roles, in order to make timely and appropriate referrals for consumers, families, carers and supporters
- identify gaps in knowledge, and locate relevant information or guidance
- develop relationships with other organisations and people to understand offerings, referral pathways and access criteria to support care, support and treatment
- advocate for partnerships between organisations that will support outcomes for consumers, families, carers and supporters
- plan care, support and treatment in collaboration with other service providers, consumers, families, carers and supporters to facilitate integrated care and improved outcomes
- advocate where system deficiencies and service gaps are identified to support access to effective services.
Technical or specialist roles
Those in technical or specialist roles will:
- guide or provide direction as to the range of services and supports available
- include online and available technological solutions when considering referral and support options
- establish inter- and intraprofessional partnerships and networks to facilitate stronger referral pathways, collaboration and consumer outcomes
- support peers to determine suitable referral and support options, engaging with other service providers
- contribute discipline-specific skills to multidisciplinary/interdisciplinary team practice
- identify barriers to systems’ work and support teams to address these.
Leadership roles
Those in leadership roles will:
- guide or provide direction on navigating the system in order to meet complex needs
- possess detailed subject matter expertise on sector policies, guidelines and relevant legislation
- draw on this detailed knowledge to deliver evidence-informed solutions to complex problems
- create partnerships with other organisations and services to deliver outcomes for consumers, families, carers and supporters
- lead commissioning and development of service-level partnerships
- contribute to innovative models of clinical governance
- act as a point of contact for stakeholder management when complex legal, risk and information sharing matters arise
- strengthen organisational structures to facilitate collaboration and cooperation with other sectors to facilitate integrated care and improved consumers, families, carers and supporters.
Reflective practice questions
- What am I doing to build my knowledge and understanding of the system and how it can support outcomes for people I work with?
- What am I doing to identify service gaps and contribute to the development of innovative responses?
Care, support and treatment uses critical reflection to recognise the interpersonal dynamics, assumptions and patterns that may arise when working with consumers, families, carers and supporters.
Outcome statements
Consumer outcome statement
I am supported by a workforce that is thoughtful, considered and continually learning. Together, we reflect on care, support, information and treatment, and the extent to which this reflects my needs, preferences and goals.
Those who provide me with care, support, information and treatment are honest with me. They always strive to better support me and my family, carers, and supporters.
Those who provide me with care, support, information and treatment seek ongoing feedback about how I experience their support. They make improvements in response to my feedback.
Carer and family outcome statement
We are supported by a workforce that is thoughtful, considered and continually learning.
The workforce reflects on ways of working by discussing ideas with us and acknowledging when they make a mistake.
They seek our feedback about how we experience their support. They make improvements in response to feedback.
Workforce outcome statement
We are thoughtful, considered and reflective in all interactions.
We are committed to excellence in service delivery and work within the scope of our skills, knowledge and capacity. We are committed to ongoing regular learning and development and understand the importance of tailored approaches to care.
We critically reflect on our actions individually, with our colleagues, and with those we support. We do this regularly and routinely to continuously improve the outcomes we deliver in collaboration with consumers, families, carers, and supporters.
Collective outcome statement
Together, we contribute to a system that supports, recognises, responds to, and reflects on the unique needs of everyone engaged in the mental health and wellbeing system.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- the importance of ongoing, regular and supportive reflection, learning, peer support and debriefing
- how to use personal values and ways of thinking to inform choices, actions and engagement with others
- how to work supportively with diverse communities
- the ways in which personal context and experience can influence practice and how these can be managed
- the importance of utilising supportive processes to promote self-care and workplace resilience
- the need to be supported and be open to ongoing learning and seek regular supportive process to achieve this.
The mental health and wellbeing workforce will:
- seek regular reflective practice to explore their own values and experience. This includes how they influence our engagement with consumers, families, carers and supporters
- seek advice and support from others, and contribute to a culture of feedback and continuous improvement
- seek out learning opportunities, including advice and support from others
- contribute to a culture of feedback, learning and continuous improvement
- use regular supportive practices including supervision, training, reflective practice or other suitable means
- recognise when peers, colleagues and others need support and provide encouragement and guidance to seek it
- practice self-care to maintain mental health and wellbeing.
Care, support and treatment role
Those in care, support and treatment roles will:
- engage in regular formal and informal opportunities for reflective practice and supervision
- actively seek supportive processes to consider the ways in which values, experiences, assumptions, power, culture, diversity, and circumstances inform work practices and work to promote best outcomes for consumers and their families
- reflect and act on limitations in knowledge and experience
- reflect on interpersonal dynamics and the quality and capacity of the relationship to support wellbeing and recovery
- reflect on disruptions or ruptures within relationships between consumers, families, carers and supporters, using this as an opportunity for growth and healing
- reflect on ways to support continuity of care, transitions and endings with consideration of their own role in using these processes to support wellbeing and recovery
- recognise and reflect on dynamics within relationships, working to promote safe, respectful and collaborative relationships between consumers, families, carers, supporters and the worker, to support wellbeing and recovery.
Technical or specialist roles
Those in technical or specialist roles will:
- deliver and/or provide expert guidance and direction on reflective practice and supervision
- seek appropriate training and support to deliver supportive reflective practice and supervision
- ensure that delivery of reflective practice and supervision is allocated and happens on a regular basis
- seek feedback on supervisory processes with the workforce that are involved
- ensure that supervisory and reflective practices are both strengths based and trauma informed
- support and guide understanding of safe and supportive ways of working
- support and guide peers to embed reflective practice into care, support and treatment
- facilitate inter- and intra-professional reflective practice groups
- facilitate discipline, cohort or other specific professional practice supervision for individuals and/or groups
- understand and be mindful of the importance of safeguarding and professional codes of practice when undertaking supervision and reflective practice
- understand and respond to varying levels of experience in the workforce with a focus on supporting ongoing careers and development.
Leadership roles
Those in leadership roles will:
- foster safe and supported working environments with strong leadership and a culture of collaboration and learning
- ensure that reflective ways of working and supervision practice are embedded across the system. This includes defining what these practices involve, their aim and how they support the design and delivery of care, support and treatment
- support resourcing and enable access to regular ongoing reflective practice and supervision for the workforce
- develop policy and procedures to support service-wide supervision and reflective practices
- model reflective and collaborative leadership, acting as a resource rather than an expert
- embed reflective ways of working by developing and resourcing formal and informal support structures and processes
- implement initiatives or strategies of positive mental health and wellbeing for all members of the workforce
- promote lived experience as a learning resource
- provide meaningful opportunities for reflective practice and ongoing learning.
Reflective practice questions
- How do I create space and time for myself, individually and with others, to think about my approaches and responses to improve my practice?
- How do I engage people around me with different skills and knowledge to support my perspectives on an issue?
Care, support and treatment is informed by current and emerging evidence. It is underpinned by active, ongoing evaluation of quality and effectiveness. Evidence is drawn from multiple sources, including lived and living experience expertise.
Outcome statements
Consumer outcome statement
I am proactively included in planning, developing and embedding new, inclusive, innovative and evidence-informed approaches.
My perspective, feedback and expertise guide the development, implementation, evaluation and continual improvement of care, support and treatment.
Carer and family outcome statement
Our experiences, expertise and knowledge are valued. We are proactively included in planning, developing, embedding and evaluating new inclusive and innovative treatment options.
Our ideas, experiences, and feedback are valued and considered both as part of our care, and as part of building a better system.
Workforce outcome statement
We are open to learning from all consumers, families, carers, and community members about their lived and living experiences. We are guided by their knowledge and changing needs.
We learn from them and drive continuous improvement, informed by evidence. We think innovatively to deliver better outcomes for consumers, their families, carers and supporters, and ourselves.
Our ideas and insights are valued and considered as a key part of building a better system.
Collective outcome statement
Together, we contribute to a system that recognises and implements research and practice insights to allow better outcomes, care, support and treatment throughout the workforce.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understand:
- that the entire mental health and wellbeing workforce is responsible for improving outcomes for consumers, families, carers, supporters and one another
- the importance of embedding emerging practice and needs, as well as evidence-based research and practice
- that the mental health and wellbeing system will continue to evolve, requiring flexibility and adaptability from the whole mental health and wellbeing workforce
- that lived experience is valued and fundamental to ethical, respectful and successful continuous improvement
- that co-production has consumers, cares, families and supporters involved in, or leading, defining the problem, designing and delivering the solution, and evaluating the outcome
- that all expertise is valuable and must be evaluated in context.
The mental health and wellbeing workforce will:
- embrace a growth mindset, demonstrating curiosity and a commitment to continuous learning, improvement, and knowledge sharing, acknowledging that setbacks may support development
- embrace learning and professional development to drive improvement and consistency
- embrace digital technologies and tools to improve care, support and treatment
- embrace evidence-informed and data-driven decision-making, recognising the many varied forms of data, including the experiences of consumers, families, carers and supporters
- recognise and address barriers to change and continuous improvement at an individual, organisational and system level
- respectfully and constructively challenge existing processes, strategies and decisions where appropriate
- promote innovation and continuous improvement, seeking out resources and strategies to improve the quality and effectiveness of services and supports
- seek to develop their skills in co-design and co-production
- consider the relevance to, and impact of, all research or continuous improvement initiatives on consumers, families, carers and supporters. Openly and honestly discuss these with the relevant people.
Care, support and treatment roles
Those in care, support and treatment roles will:
- identify areas for improvement and champion strategies for improvement
- recognise service and system barriers that affect outcomes for certain groups and develop strategies to mitigate these
- drive improved mental health and wellbeing outcomes for consumers, families, carers and supporters using evidence-informed decision-making
- participate in research and knowledge translation and dissemination activities to embed evidence into practice.
Technical or specialist roles
Those in technical or specialist roles will:
- use data to identify trends and patterns and translate this into accessible messaging that is easily understood
- translate complex data and information into insights and continuous improvement
- look for opportunities to share evidence with the broader workforce
- consider using co-production for service improvement projects
- build and communicate a compelling narrative around change and continuous improvement
- drive improved mental health and wellbeing outcomes for at-risk cohorts. These include Aboriginal people, and people disadvantaged by geographical location, socioeconomic circumstances, disability and other factors
- develop, implement and measure the extent to which care, support and treatment delivers improved health and wellbeing outcomes
- develop, implement and measure strategies that address social determinants of health
- systematically monitor and evaluate the service, consistent with the national standards for mental health services to ensure the best possible outcomes for consumers, carers, family members and/or supporters.
Leadership roles
Those in leadership roles will:
- drive a continuous improvement agenda through prioritising reviews and developing practical strategies for improvement
- develop an organisational culture that actively creates opportunities to improve, for example, by facilitating joint academic or clinical partnerships
- monitor and report on service demand, needs and provision, including effectiveness of outcomes, to inform future service improvement
- ensure all members of the workforce have access to relevant research evidence and the skills to interpret, appraise and use it in their work
- drive improved health and wellbeing outcomes for the workforce
- embed lived experience in service planning, delivery and improvement, as well as in the design and delivery of professional development activities and workforce capability
- identify leadership potential and support its development
- support the iterative development and implementation of new ideas, initiatives and service delivery
- drive cultures to support research and continuous improvement, and remove barriers, for example through time-release, funding and mentoring
- support the development of evaluation measures and implementation of evaluation frameworks
- encourage the use of innovative and evidence-based approaches
- maintain focus across immediate, medium and long term, to ensure staff and services are evolving with needs
- translate innovative ideas into practice and promote system-wide adoption
- support system-level adoption of consistent methods of collection and collation of data and information
- translate insights into meaningful system-based recommendations and change.
Reflective practice questions
- How is my practice informed by current and emerging research?
- How is my practice informed by lived experience?
- How do I create time to improve the way I am working, and supporting others to do this?
- How do I develop my capacity to use evidence in my work?
- How do I help others to build capacity or access resources to use evidence in their work?
- How do I invite ongoing feedback and integrate it into my approaches?
Care, support and treatment uses online and other digital technologies to improve mental health and wellbeing. This includes access to information, service delivery, education, promotion and prevention. Services, teams and practitioners use digital technologies to enable accessible, holistic, person-centred and integrated care. Technologies may include apps, portals, social media, smartphones, augmented or virtual reality, wearables, activity tracking, e-referral, notifications and artificial intelligence.
Outcome statements
Consumer outcome statement
I am informed and make choices about the digital technology options available to me, including benefits, risks and limitations, in relation to my care, treatment and support.
I lead decisions about the use of digital tools and technologies available to me. I have flexibility in how I access and use them.
Carer and family outcome statement
We are supported to understand and access digital tools and technologies to assist the person we support and ourselves. This includes knowing and understanding the risks and benefits of using digital technologies.
We understand how these tools can assist in including us in the delivery of care and in our own wellbeing.
Workforce outcome statement
We receive appropriate training, education and resources to confidently and capably use technology to enhance our practice and service provision.
We use our expertise in digital technologies to assess and mitigate risks to consumers and carers. We assess levels of digital literacy to match care with the needs of consumers, carers and families.
We use technology to enable, complement and enhance our practice or service provision, as appropriate.
Collective outcome statement
Together, we contribute to a system that uses digital technologies to deliver care, support and treatment to consumers, families, carers and supporters.
Key knowledge and skills
Whole of mental health and wellbeing workforce
The mental health and wellbeing workforce understands:
- current privacy and security management policies and legislation
- the risks and benefits of using digital technologies in providing support, and the need to make informed decisions about their use in care, support and treatment
- consumer information collection, privacy and storage responsibilities, including the use of relevant mental health and wellbeing systems for electronic data management
- the importance of using different digital technologies and supports to facilitate increased access, communication and outcomes regarding care, support and treatment
- health and digital literacy are linked to mental health and wellbeing outcomes for consumers.
The mental health and wellbeing workforce will:
- maintain contemporary skills in the use of information technology, keeping up to date with emerging technologies and trends that can support practice
- champion the use of innovative technologies in the workplace, recognising that the digital landscape is rapidly evolving
- adapt modes of communication and engagement to the consumer’s preferences, and with consideration of the needs of their family, carers and supporters
- draw on a range of digital tools and technologies, including the use of apps, and video conferencing that support communication, access and engagement
- use secure and appropriate digital technologies and tools, including electronic messaging systems, and video conferencing that support collaboration between providers.
Care, support and treatment roles
Those in care, support and treatment roles will:
- draw on a range of digital tools and technologies to complement or support assessment, care planning, referrals and collaboration
- seek out, identify and use digital tools and technologies to complement or provide care, support and treatment
- use digital tools and technologies to complement or provide care, support and treatment
- use evidence-informed judgement as to when digital tools and technology are suitable or appropriate, and identify, manage and mitigate risks associated with their use
- consider the most appropriate technological solutions when collaboratively identifying referral and support options.
Technical or specialist roles
Those in technical or specialist roles will:
- guide understanding of, and champion use of, digital tools and technologies to complement or provide care, support and treatment
- contribute to innovations in the use of technology to support care, support and treatment
- use technology to support continuous improvement and enhancements in access to and delivery of care, support and treatment.
Leadership roles
Those in leadership roles will:
- embed digital tools and technologies across the system, including in the delivery of care, support and treatment
- advocate for the benefits of digital technologies in delivering outcomes
- embed digitally safe ways of working, safeguarding against risks associated with digital tools and technologies, for example, data privacy
- provide meaningful opportunities for ongoing learning that promote the use of digital tools and technologies in practice
- guide and support appropriate use of systems for mental health and wellbeing data collection, to support practice and/or translational research.
Reflective practice questions
- How do I use digital technologies to facilitate and support engagement with consumers, families, carers and supporters?
- How do I understand digital literacy as it applies to the people I support?
- How do I mitigate risks when using digital technology?
Updated